Diet and kwashiorkor: a prospective study from rural DR Congo
A peer-reviewed article of this Preprint also exists.
Author and article information
Abstract
The etiology of kwashiorkor remains enigmatic and longitudinal studies examining potential causes of kwashiorkor are scarce. Using historical, longitudinal study data from the rural area of Bwamanda, Democratic Republic of Congo, we investigated the potential causal association between diet and the development of kwashiorkor in 5 657 preschool children followed 3-monthly during 15 months.We compared dietary risk factors for kwashiorkor with those of marasmus. Kwashiorkor was diagnosed as pitting oedema of the ankles; marasmus as abnormal visibility of skeletal structures and palpable wasting of the gluteus muscle. A food frequency questionnaire was administered 3-monthly to record the consumption of the 41 locally most frequent food items. We specified Hanley-Miettinen smooth-in-time risk models containing potential causal factors, including food items, specialmeals prepared for the child, breastfeeding, disease status, nutritional status, birth rank, age, season and number of meals. Bayesian Information Criteria identified the most plausible causal model of why some children developed kwashiorkor.In a descriptive analysis of the diet at the last dietary assessment prior to development of kwashiorkor, the diet of children who developed kwashiorkor was characterized by a low intake of sweet potatoes, papaya and “other vegetables” [0.0% , 2.3% (95%CI: 0.4, 12.1) and 2.3% (95%CI: 0.4, 12.1)] in comparison with children who did not develop kwashiorkor [6.8% (95%CI: 6.4, 7.2), 15.5% (95%CI: 15, 16.1) and 15.1% (95%CI: 14.6, 15.7)] or children who developed marasmus [4.5% (95%CI 2.6, 7.5) 11.8% (95%CI: 8.5, 16.0) and 17.6% (95%CI: 13.7, 22.5)]. Sweet potatoes and papaya have high β-Carotene content and so may some of “the other vegetables”. We found that a risk model containing an age function, length/height-for age Z-score, consumption of sweet potatoes, papaya or other vegetables , duration of this consumption and its interaction term, was the most plausible model. Among children aged aged 10-42 months, the risk of developing kwashiorkor increased with longer non-consumption of theses foods.The analysis was repeated with only children who developed marasmus as the reference series, yielding similar results. Our study supports that β-Carotene may play an important role in the protection against kwashiorkor development.
Cite this as
2013. Diet and kwashiorkor: a prospective study from rural DR Congo. PeerJ PrePrints 1:e119v1 https://doi.org/10.7287/peerj.preprints.119v1Author comment
This article is under review in PeerJ.
Sections
Supplemental Information
Age distribution, length/height-for-Age Z-score (HAZ), and Weight for Length Z-score (WLZ) and for children with different clinical nutritional status
Age distribution, length/height-for-Age Z-score (HAZ), and Weight for Length Z-score (WLZ) and for children with different clinical nutritional status. Z-scores based on the WHO-2006 Child Growth Standards[15].
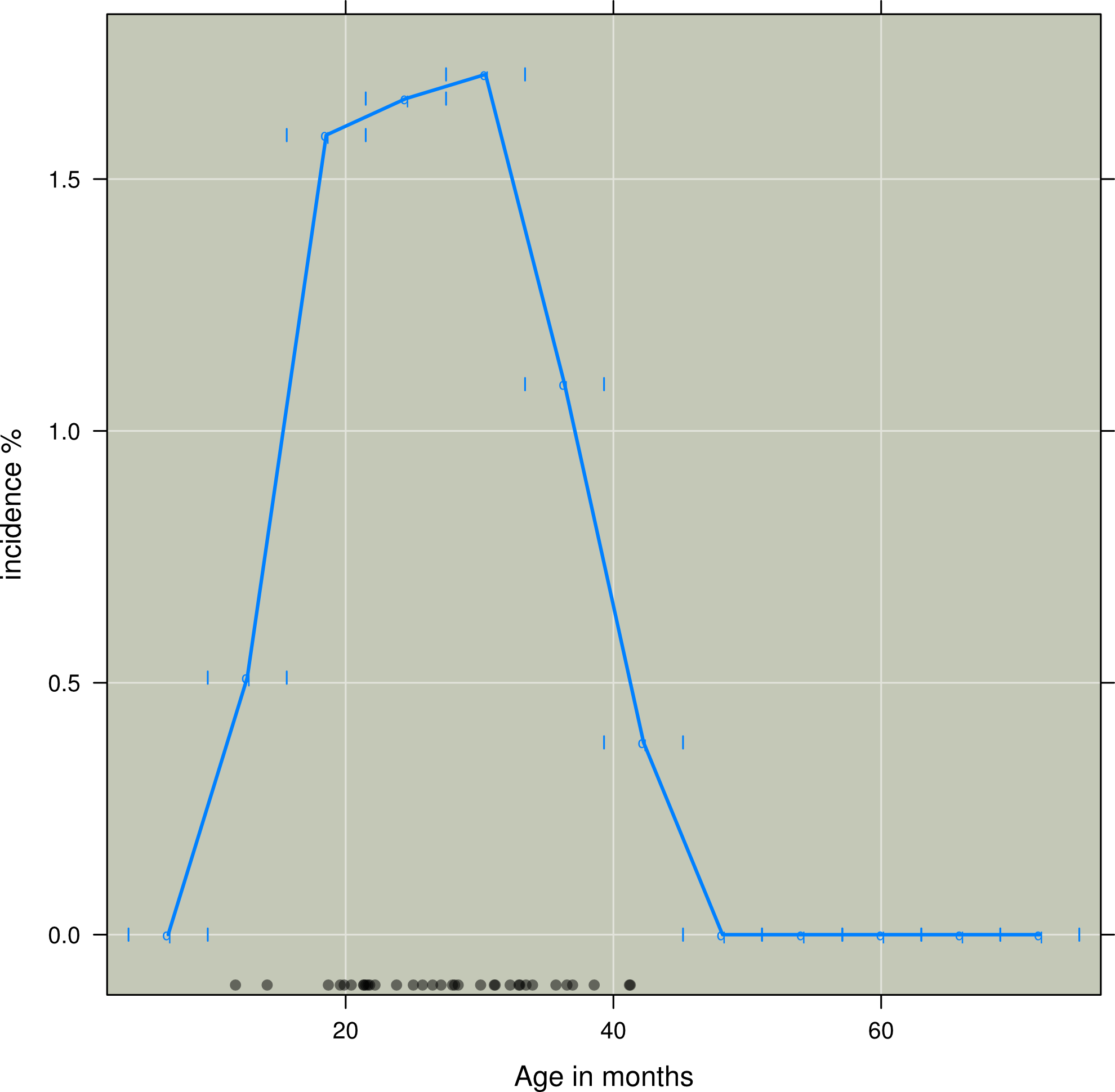
Three months incidence of kwashiorkor according to age in months in intervals of six months
Incidence of kwashiorkor (y-axis) against age in months (x-axis). Black dots indicate age of those children which developed kwashiorkor
Consumption of different food items in the survey round preceding the development of kwashiorkor and non-development of kwashiorkor and development of marasmus
Consumption of different food items in the survey round preceding the development of kwashiorkor (n = 37) and non-development of kwashiorkor (n = 8108) and development of marasmus (n=374) in children between 6 and 50 months of age. * denotes p-value < 0.05, while** denotes p-value<0.01 with the value estimated using 2-sample test for equality of proportions with continuity correction as implemented in the prop test in R
The coefficients for the non-proportional hazard model with person moments sampled from the entire population
The Age variable is a transformation based on the distribution of kwashiorkor across age. T is a variable that describes the duration of consuming a food item containing β-Carotene. PaSV is a variable that combines papaya, other vegetables and sweet potatoes and weighted by the β-Carotene content of 100 g of the item. The Height-for-Age Z-score (HAZ) are based on the WHO-2006 Child Growth Standards
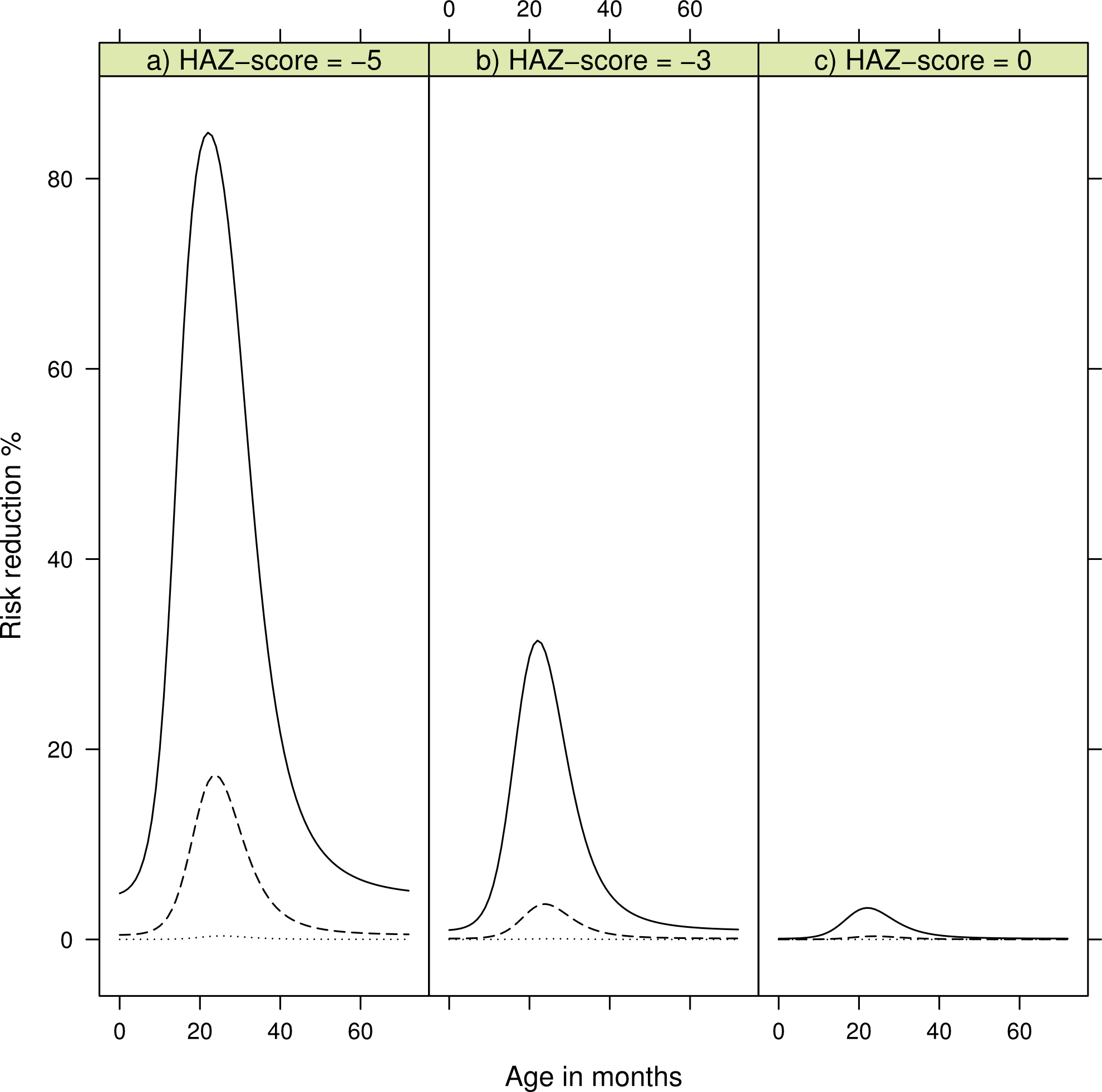
Risk reduction for developing kwashiorkor reduction of consuming β-Carotene rich products according to age in months
Dotted line is risk reduction after two months, dashed line after four months, and solid line after six months. Panel a) shows risk reduction for a child with a Height-for-Age Z-score (HAZ) of minus five, b) for a child with HAZ of minus three, and c) a child with HAZ of zero. HAZ-scores are based on the WHO-2006 Child Growth Standards[15].
The coefficients for the non-proportional hazard model with reference persons moments drawn from persons developing marasmus
The age variable is based on the distribution of kwashiorkor across age. T is a variable that describes the duration of consuming a food item containing β-Carotene. PaSV is a variable that includes papaya, other vegetables and sweet potatoes weighted by the β-Carotene content of 100 g of the item. Height-for-Age Z-score (HAZ) are based on the WHO-2006 Child Growth Standards[15].
Additional Information
Competing Interests
The authors have no conflicts of interest.
Author Contributions
Hallgeir Kismul analyzed the data, contributed reagents/materials/analysis tools, wrote the paper.
Jan Van den Broeck conceived and designed the experiments, performed the experiments, contributed reagents/materials/analysis tools.
Torleif Markussen Lunde analyzed the data, contributed reagents/materials/analysis tools.
Ethics
The following information was supplied relating to ethical approvals (i.e., approving body and any reference numbers):
Ethical approval for the Bwamanda study had been granted by the University of Leuven’s Tropical Childcare Health Working Group
Funding
The study was funded by Nutricia Research Foundation. The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.

{kind=link}
{kind=link}