Supply-side barriers to maternal health care utilization at health sub-centres in India
- Published
- Accepted
- Subject Areas
- Global Health, Health Policy, Nursing, Public Health, Women's Health
- Keywords
- Health Sub-Centre, India, Rural Public Health System, Auxiliary Nurse Midwives, Postnatal Care, Antenatal Care, Delivery Care, Maternal Health
- Copyright
- © 2016 Singh
- Licence
- This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, reproduction and adaptation in any medium and for any purpose provided that it is properly attributed. For attribution, the original author(s), title, publication source (PeerJ Preprints) and either DOI or URL of the article must be cited.
- Cite this article
- 2016. Supply-side barriers to maternal health care utilization at health sub-centres in India. PeerJ Preprints 4:e2362v1 https://doi.org/10.7287/peerj.preprints.2362v1
Abstract
Introduction: There exist several barriers to maternal health service utilization in developing countries. Most of the previous studies conducted in India have focused on demand-side barriers, while only a few have touched upon supply-side barriers. None of the previous studies in India have investigated the factors that affect maternal health care utilization at Health Sub-Centers (HSC) in India, despite the fact that these institutions, as the nearest available public healthcare facilities in rural areas, play a significant role in providing affordable maternal health care. Therefore, this study aims to examine the supply-side determinants of maternal service utilization at HSCs in rural India.
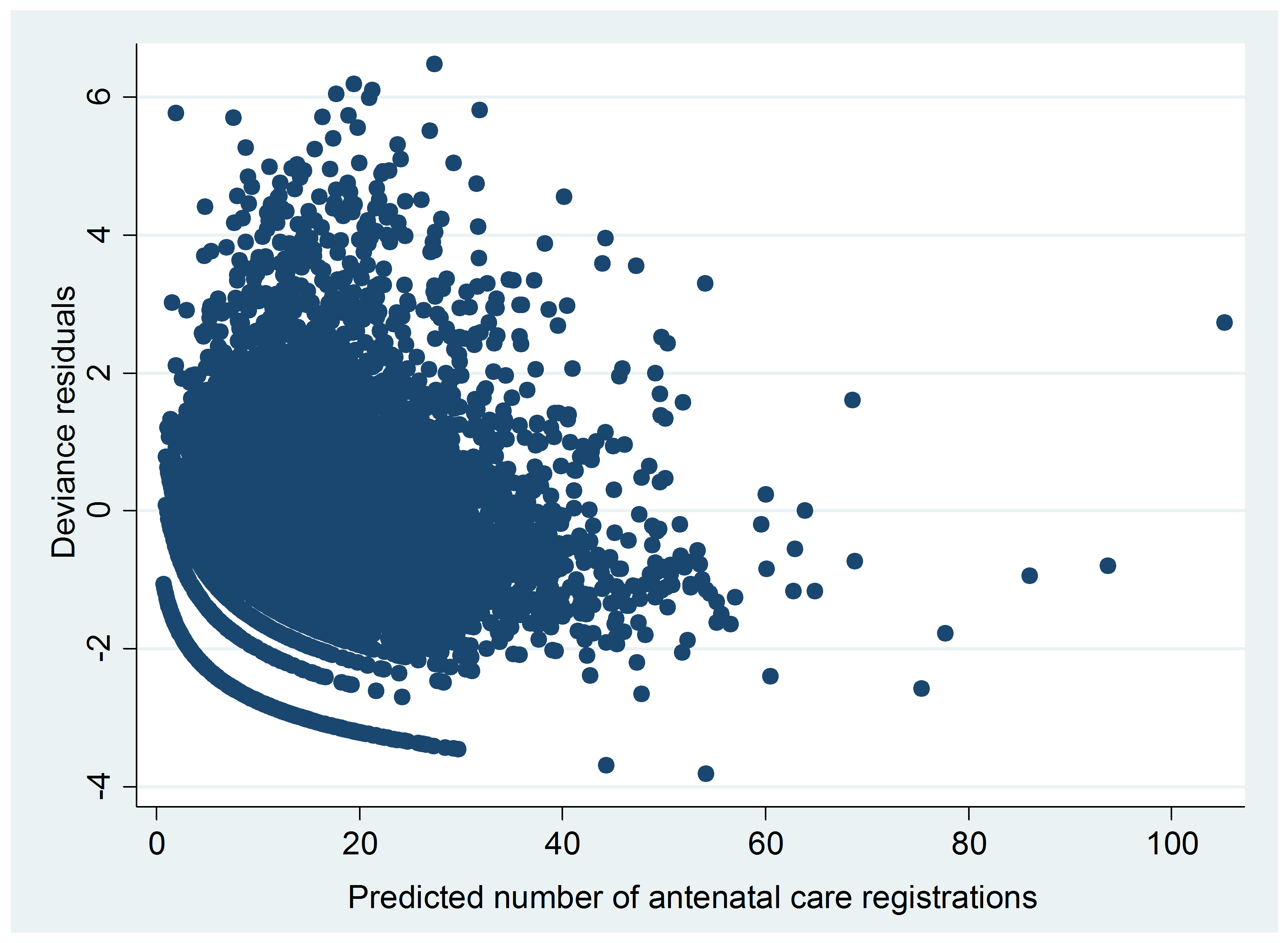
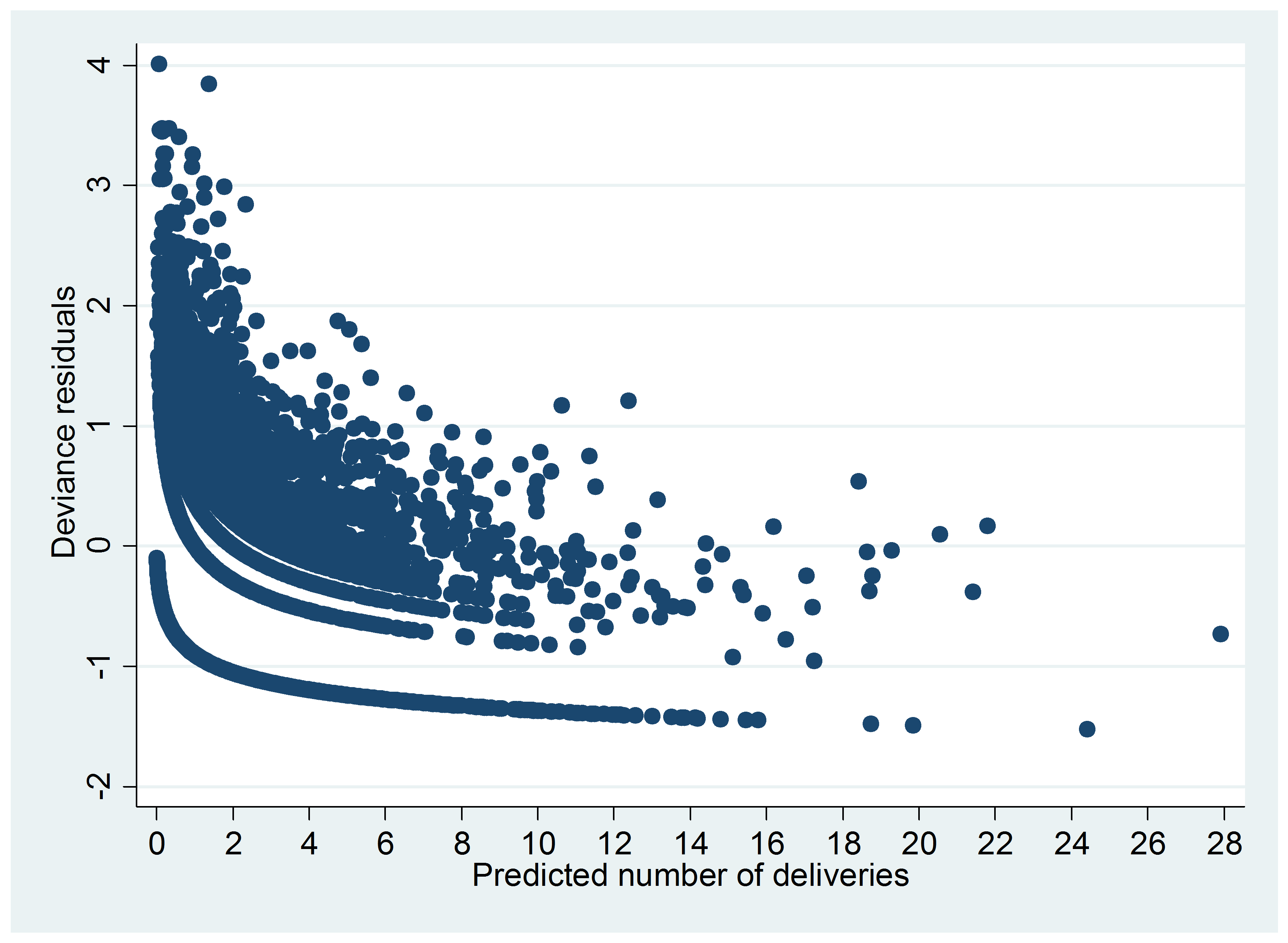
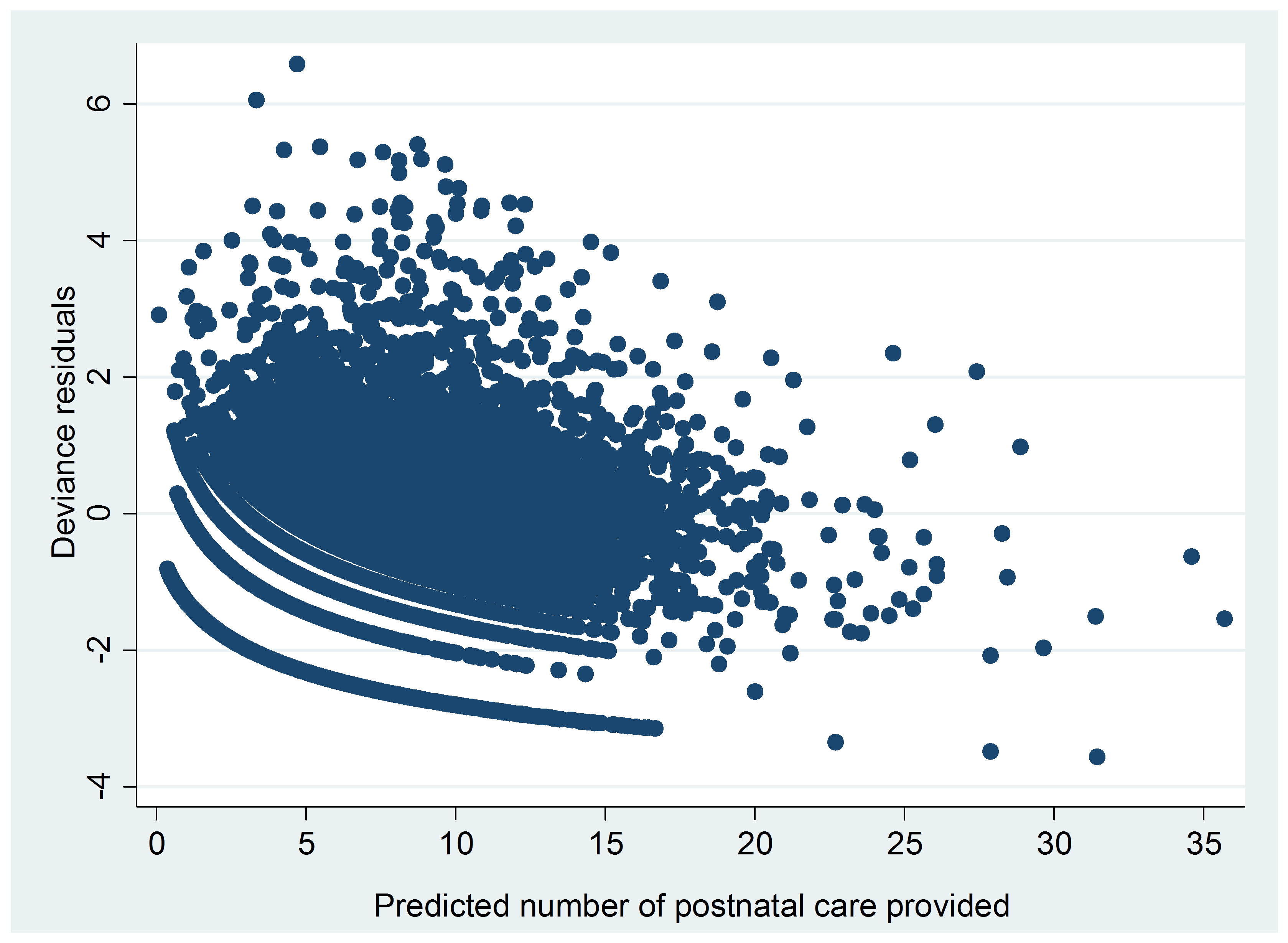
Data and Methods: This study uses health facility data from the nationally representative District-Level Household Survey, which was collected in 2007–2008 to examine the effect of supply-side variables on the utilization of maternal healthcare services across HSCs in rural India. Since the dependent variables (the number of antenatal registrations, in-facility deliveries, and postnatal care services) are count variables with considerable dispersion, the data has been analyzed using negative binomial regression instead of Poisson regression.
Results: The results show that those HSCs run by a contractual auxiliary nurse midwife (ANM) are likely to offer a lower volume of services when compared to those run by a permanent ANM. The availability of obstetric drugs, weighing scale, blood pressure equipment is associated with the increased utilization of antenatal and postnatal services. The unavailability of labor/examination table and bed screen is associated with a reduction in the number of safe deliveries and postnatal services. The utilization of services is expected to increase if essential facilities, such as water, telephone, toilet, and electricity, are available at HSCs. Monitoring of an ANM’s work by the Village Health and Sanitation Committee (VHSC) and the in-service training of ANMs appear to have a positive impact on the utilization of services. The distance of an ANM’s actual residence from the sub-center village where she works is negatively associated with the utilization of delivery and postnatal services. These findings are robust to the inclusion of several demand-side factors.
Conclusion: To improve maternal healthcare utilization at sub-centers, the government should ensure the availability of basic infrastructure, drugs, and equipment at all sub-centers. Monitoring of ANMs’ work by VHSCs could play an important role in improving healthcare utilization at the HSCs; therefore, it is important to establish VHSCs in each sub-center village. The issue of the relatively low utilization of maternity services in the HSCs that are run solely by contractual ANMs needs to be investigated further.
Author Comment
This is a submission to PeerJ for review.
{kind=link}
{kind=link}
{kind=link}