
Contributions of burning incense on indoor air pollution levels and on the health status of patients with chronic obstructive pulmonary disease
- Published
- Accepted
- Received
- Academic Editor
- Tuan Nguyen
- Subject Areas
- Public Health, Respiratory Medicine, Environmental Impacts
- Keywords
- Burning incense, Chronic lung disease, Indoor particulate matter, Lung function
- Copyright
- © 2020 Guo et al.
- Licence
- This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits using, remixing, and building upon the work non-commercially, as long as it is properly attributed. For attribution, the original author(s), title, publication source (PeerJ) and either DOI or URL of the article must be cited.
- Cite this article
- 2020. Contributions of burning incense on indoor air pollution levels and on the health status of patients with chronic obstructive pulmonary disease. PeerJ 8:e9768 https://doi.org/10.7717/peerj.9768
Abstract
Background
Among Buddhist or Taoist Taiwanese residents, burning incense is a common source of indoor particulate matter (PM), including PM10 and PM2.5, and can adversely affect the health status of patients with chronic obstructive pulmonary diseases (COPD). However, few studies have focused on the effects of intermittent burning of incense on PM concentration levels and the health status of patients with COPD. This correlational cohort study aimed to investigate the association between burning incense exposure duration, indoor air pollution levels, and lung function in patients with COPD in Taiwan.
Methods
We assessed 18 outpatients at seven time points with moderate-to-severe COPD using the COPD Assessment Test (CAT), and lung function tests. PM level changes were assessed at seven intervals using generalized estimating equations.
Results
Participants were primarily male (84%), with a mean age of 72.1 (standard deviation (SD) ± 9.3) years, and with a mean COPD duration of 3.7 (SD ± 3.1) years. Both PM10 and PM2.5 levels were the same as the background levels 1 h after incense burning. Burning incense may not influence lung function or symptom severity in patients with COPD in a short-time period. Air quality returned to baseline levels 1 h after burning incense.
Conclusion
Patients with COPD should avoid staying in rooms where incense is burnt, for up to 1 h. The small sample size and short study period may have influenced our results. Future longitudinal studies with larger sample sizes and long-term follow-ups are recommended.
Introduction
Taiwan, according to a United States 2014 international religious freedom report, 35% (approximately 8.15 million) of the Taiwanese population was Buddhist, and 33% (approximately 7.68 million) were Taoists (AIT, 2015). Burning incense forms an important aspect of worship in Buddhist and Taoist religious ceremonies in Taiwan. Moreover, most Taiwanese have a shrine at home to worship gods and ancestors, and incense is burned in the mornings and evenings. A study by Lung (2009) indicated that fine particulate matter (PM2.5) accumulation due to incense burning ranged from 75 µg/m3 to 100 µg/m3, which was 23 times higher compared to 2012 air quality recommendations for PM2.5 levels of 35 µg/m3, as declared by the EPA (2012). Moreover, Chen, Mao & Lin (1999) found that, on average, Taiwanese people spent 70–90% of their time indoors. Therefore, long-term exposure to indoor air pollution among Taiwanese people is likely to result in adverse health risks.
Air pollution may cause respiratory diseases, and lung exposure to air pollution is reported to be one of the major environmental risk factors for respiratory inflammation (Wang et al., 2007; WHO, 2018a). Over the last decade, the prevalence of respiratory diseases has been reported to have increased, and respiratory diseases were reported to be the third leading global cause of death in 2016 (World Health Organization, 2018a; World Health Organization, 2018b). Chronic obstructive pulmonary disease (COPD) is an incurable disease, characterized with chronic blockage of airflow and gradually worsening lung function (World Health Organization, 2017), resulting from respiratory inflammation.
Some studies have demonstrated that the emission of fine PM with an aerodynamic diameter of <2.5 µm due to burning incense involves toxic chemicals such as heavy metals and polycyclic aromatic hydrocarbons (Chao, Lin & Hsieh, 1997; Pan et al., 2014). Fang et al. (2002) investigated the distribution of the aerodynamic diameter of PM2.5 according to micro-orifice uniform deposited impactor (MOUDI) results, and found an elevated level due to an increase in incense burning during peak dates on the 1st and 15th days of the Chinese calendar. Fang et al. (2002) also found that PM2.5 was the principal emission particulate resulting from incense burning and was harmful to health because it entered pulmonary alveoli via inhalation. One study undertaken in Singapore reported that people with a habit of incense use, or exposure to an incense burning environment over a long period of time, showed a 12% higher fatal risk of cardiovascular diseases compared to those without such use or exposure (Pan et al., 2014). Two studies found an association between incense burning and lung function, indicating that the higher the frequency of incense use, the lower the lung function (Hsu, 2006; Wang, 2008). A prospective cohort study undertaken in Singapore demonstrated that long-term exposure to incense burning was associated with squamous cell carcinoma of the respiratory tract, with an especially increased risk in women (Friborg et al., 2008).
Although incense burning is known to be associated with respiratory diseases related to morbidity and mortality, few studies have explored the PM concentration levels resulting from burning incense or the association between incense burning, the health status of patients with COPD (Friborg et al., 2008; Chuang et al, 2011, and the indoor PM concentration over specified periods of time. To our knowledge, this is the first study to investigate this type of association. This study aimed to determine the PM10 and PM2.5 concentration levels from incense burning in the home environment, as well as the lung function and health status in patients with COPD. Moreover, this study investigated the time it took for background concentrations of PM10 and PM2.5 to recover to original levels following incense burning emissions. Our findings may provide guidance for patients with COPD who regularly engage in incense burning, to reduce the risk of morbidity due to respiratory diseases resulting from exposure to an incense burning environment.
Materials & Methods
Study design and participant recruitment
In this cohort study comprising 18 participants, we examined responses to a lifestyle behavior questionnaire, namely, the Chronic Respiratory Questionnaire, and the results of a lung function test. In addition, changes in PM in the home were assessed at 7 time points (baseline, 10-, 20-, 30-, 60-minutes, 3 h, and 5 h). Outpatients with COPD were recruited from a regional hospital in the south-western region of Taiwan. Inclusion criteria comprised the following: age ≥40 years; a chest physician made the diagnosis according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD), which presents of a post-bronchodilator FEV1/FVC <0.70; moderate-to-severe COPD according to the GOLD grades (30 <FEV1 predicted <80%) (Agusti & Vogelmeier, 2019); the habit of burning incense and having a shrine at home, and being able to understand and communicate in Mandarin or Taiwanese. Exclusion criteria comprised the following: heart diseases, cancer (any type), pulmonary tuberculosis, or asthma. This study was approved by the Institutional Review Board Ethics Committee of Chang Gung Memorial Hospital (102-2417B). After explaining the study aims and procedures to potential participants, informed consent was obtained from all participants agreeing to participate in the study. After written informed consent was obtained, data were collected via home visits involving face-to-face interviews using structured questionnaires, and environmental data were collected through observations and using specialized equipment.
Participants
To the best of our knowledge, no study has reported changes in particulate matter (i.e., PM2.5 or PM10) after burning incense among COPD patients. Therefore, we assumed the level of PM2.5 increases from 200 µg/m3 before burning incense to 400 µg/m3 immediately after burning incense with a common standard deviation of 200 µg/m3; a minimum of 15 subjects were required to achieve an alpha level of 5% and a power level of 90%. Twenty participants were initially included in the study; however, 2 participants withdrew their consent, and were subsequently excluded, during the study period as their disease had exacerbated and they were admitted to hospital. There was no statistically significant difference between included (N = 18) and excluded (N = 2) participants in terms of variables such as age, body mass index (BMI), and length of COPD duration except COPD severity. Among 18 participants, no data were missing for any variable or time point.
Measurements and instruments
Data were collected for 30–45 min, using structured questionnaires to determine demographic and clinical characteristics, and assessed using a COPD Assessment Test (CAT) and a modified British Medical Research Council dyspnea scale (mMRC). We also collected environmental characteristics and air quality assessments including PM10 and PM2.5 concentration levels using an aerosol spectrometer (Model TSI8532).
Demographic and clinical characteristics
Demographics included age, sex, weight status, employment status, education levels, exercise habits, smoking status, disease severity, BMI, and a waist-hip ratio. Clinical characteristics were assessed in relation to the Charlson comorbidity index (CCI), the number of years since the COPD diagnosis (duration of disease), and forced expiratory volume in 1 s (FEV1). The CCI is used as a measure of 1-year mortality risk and consists of 18 comorbidities (Charlson et al., 1987). The CCI scoring scales range from 0 (without any symptoms) to 6, with higher CCI scores indicating a higher disease burden level.
The forced expiratory volume in one second (FEV1)
As COPD progresses, FEV1 tends to decline gradually. A pulmonary function test, a non-invasive test, and measurements such as FEV1 and forced vital capacity (FVC) are used to diagnose COPD and determine its severity based on American Thoracic Society (ATS), European Respiratory Society (ERS), and GOLD grades (Agusti & Vogelmeier, 2019; Celli et al., 2015; Jo et al., 2018). A change in pulmonary function is also useful to determine the influence of risk factors on COPD exacerbation (Vestbo & Lange, 2016; Scanlon et al., 2000).
The COPD Assessment Test (CAT)
The COPD Assessment Test (CAT) was designed to estimate the condition of COPD symptoms, including cough, phlegm (mucus), chest tightness, breathlessness while climbing a hill or stairs, limitation to activity at home, confidence, while leaving home, sleep quality, and energy. The score of each item is from 0 to 5 in the CAT, and the total score ranges from 0 to 40. A higher CAT score denoted poorer health status in terms of COPD (Agusti & Vogelmeier, 2019; Jo et al., 2018). In this study, the Chinese version of the CAT (CAT-Chinese version) was adopted. The Cronbach’s alpha of CAT-Chinese version was 0.81, which showed a good internal consistency, and revealed that higher CAT score indicated a greater severity of lung disease (Chai, Liu & Cai, 2011). Therefore, the CAT-Chinese version is a simple, reliable, and validated questionnaire to evaluate the symptoms of COPD patients.
The modified British Medical Research Council (mMRC) scale
The mMRC scale comprises a 5-point scale: 0 (breathlessness due to strenuous exercise), 1 (breathlessness when hurrying or walking up a hill), 2 (walking slower than people of the same age due to breathlessness), 3 (breathlessness after walking a few minutes or for 100 yards), and 4 (breathlessness when dressing). The mMRC scale is recommended for COPD assessment by the GOLD. Moreover, the mMRC scale is a predictor of future mortality risk (Agusti & Vogelmeier, 2019).
Environmental characteristics
We assessed participants’ home environment, including meteorological conditions (rain, and outdoor and indoor moisture), the smoking status of family members, the residential location, the age and type of house, the direction the house was facing and its proximity to a main road, and the frequency of having windows and doors open.
Air quality assessment
All study participants were in the habit of burning incense, and all participants had a shrine at home. Air sampling for PM10 and PM2.5 concentration levels due to incense burning was measured at the shrines, using an aerosol spectrometer (Model TSI8532). The PM10 and PM2.5 levels were assessed at 3 time points, each at 1-minute intervals; and the average value of the 3 measurements was used as the outcome for each specific assessment. Furthermore, PM10 and PM2.5 assessments were undertaken during seven time intervals as follows: a pre-test assessment prior to burning incense; at 10-, 20-, 30-, and 60-minute intervals during the burning of the incense; and at 3 h and 5 h after incense burning had stopped. CAT and mMRC scores were determined and lung function tests were performed after each time interval. The normal values of daily PM2.5 & PM10 levels as stated by the Taiwan Environment Protection Administration are 35 µg/m3 and 125 µg/m3, respectively (EPA, 2012).
Statistical analyses
The SPSS 25 package (IBM SPSS Inc., Chicago, IL) was used to analyze data. The characteristics of the study participants, house types, residential locations, and home environments (in relation to incense burning) are presented as numbers and percentages for categorical variables or as means and standard deviations for continuous variables. Some studies have reported their findings concerning PM indoor concentrations relative to external levels, different cooking methods (Isaxon et al., 2015), smoking, incense (Wallace et al., 2003), and candles (Beko et al., 2013). Moreover, house type and window opening can be to correlated to indoor PM concentrations (Shao et al., 2019; Andersen et al., 2011). A recent comprehensive literature review showed that the main origin of PM2.5 and PM10 at home was due to outdoor air (Morawska et al., 2017). Therefore, covariates such as house types, whether windows are open or not, family members who actively smoke, and outdoor PM were collected based on previous studies. The effect of burning incense on PM2.5 and PM10 was assessed using a generalized estimating equation (GEE) model with a robust standard error and an exchangeable working correlation matrix for the adjustment of time (Liang & Zeger, 1986). In the GEE analysis, the linking function was identity, and the distribution was normal. Since there were only 18 participants, covariate adjustment may not have been feasible, and therefore, the only explanatory variable in the GEE model was the time effect. In the GEE analysis, we compared baseline values to those taken after burning incense. To evaluate the robustness of the GEE model, we changed the linking function to log and the distribution to gamma.
Results
Participant characteristics
Table 1 indicates the demographics of participants in our study. This study recruited 18 participants, who were mostly male (88.9%). The average age was 75.1 (± 8.6) years. The average BMI and waist-hip ratio were 24.2 (± 2.1) kg/m2, and 95.9 (± 6.4) %, respectively. Additionally, the average duration of COPD and the mean predicted FEV1 were 5.1 (± 4.3) years and 54.1 (± 14.2), respectively. Five participants (27.8%) reported exercising regularly. The average distance that participants accomplished in the 6-minute walking test was 135.2 (± 136.9) meters.
| Variable | N (%) or Mean ± SD |
|---|---|
| Residential area location | |
| Downtown | 3 (16.7) |
| Rural area | 15 (83.3) |
| House age (years) | 45.6 ± 25.3 |
| House types | |
| Single-family home | 5 (27.8) |
| Townhouse | 3 (16.7) |
| Courtyard house (included siheyuan) | 10 (55.6) |
| Nearby main road | |
| No | 11 (61.1) |
| Yes | 7 (38.9) |
| Frequency of opened windows | |
| Opened frequently | 14 (77.8) |
| Closed frequently | 2 (11.1) |
| Irregularly | 2 (11.1) |
| Variable | N (%) or Mean ± SD |
| Smoking status of family members | |
| No | 14 (77.8) |
| Yes | 4 (22.2) |
| Weather condition (rain) | |
| No | 14 (77.8) |
| Yes | 4 (22.2) |
| Outdoor moisture | 67.4 ± 10.4 |
| Indoor moisture | 68.2 ± 10.3 |
| House facing direction | |
| North | 1 (5.6) |
| West | 2 (11.1) |
| Unknown | 15 (83.3) |
In terms of weight status, 7 (38.9%) participants were of normal weight and 11 (61.9%) were overweight/obese. With regard to education levels, 2 (11.1%) participants were uneducated, 13 (72.2%) had graduated from elementary school, and 3 (16.7%) had graduated from junior high school or above. Concerning smoking status, 3 (16.7%) participants were non-smokers, 14 (77.8%) were former smokers, and 1 (5.6%) participant was an active smoker. Based on the Taiwan Society of Pulmonary and Critical Care Medicine COPD guidelines (TSPCCM, 2017), the COPD severity concerning 14 participants (72.2%) was moderate, 3 (22.2%) participants had severe COPD, and 1 (5.6%) participant had very severe COPD.
Home environment (including house type and residential location)
Table 2 shows the characteristics of the home environment. Most participants resided in rural areas (83.3%) and opened their windows and doors during the day (77.8%). Most houses were located near low-traffic roads or in lanes where there was a lower risk of harmful PM from traffic emission.
| Variable | N (%) or Mean ± SD |
|---|---|
| Gender | |
| Male | 16 (88.9) |
| Female | 2 (11.1) |
| Age (years) | 75.1 ± 8.6 |
| BMI (kg/m2) | 24.2 ± 2.1 |
| Waist-hip ratio (%) | 95.9 ± 6.4 |
| Weight status | |
| Normal | 7 (38.9) |
| Overweight | 9 (50.0) |
| Obese | 2 (11.1) |
| Employment status | |
| Part-time job | 2 (11.1) |
| Retired | 16 (88.9) |
| Exercise habit | |
| No | 13 (72.2) |
| Yes | 5 (27.8) |
| Education level | |
| Uneducated | 2 (11.1) |
| Elementary school | 13 (72.2) |
| Junior high school or above | 3 (16.7) |
| Smoking status | |
| Never | 3 (16.7) |
| Quit | 14 (77.8) |
| Current smoker | 1 (5.6) |
| COPD severity | |
| Moderate | 13 (72.2) |
| Severe | 4 (22.2) |
| Very severe | 1 (5.6) |
| Charlson comorbidity index | |
| 1 | 7 (38.9) |
| 2 | 7 (38.9) |
| 3 / 4 | 4 (22.2) |
| Length of COPD duration (years) | 5.1 ± 4.3 |
| 6 min walking test (m) | 135.2 ± 136.9 |
| Forced expiratory volume in 1 s (FEV1) (%) | 54.1 ± 14.2 |
Most days were sunny (77.8%). The average outdoor moisture level was 67.4% (± 10.4%), but the average indoor moisture level was higher, at 68.2% (± 10.3%), (Table 2).
Pollutant concentrations
Our study findings showed that PM10 and PM2.5 levels were the highest 30 min after incense burning (see Figs. 1 and 2) and that PM10 and PM2.5 levels were found to be the same as background concentration levels 1 h after incense burning.
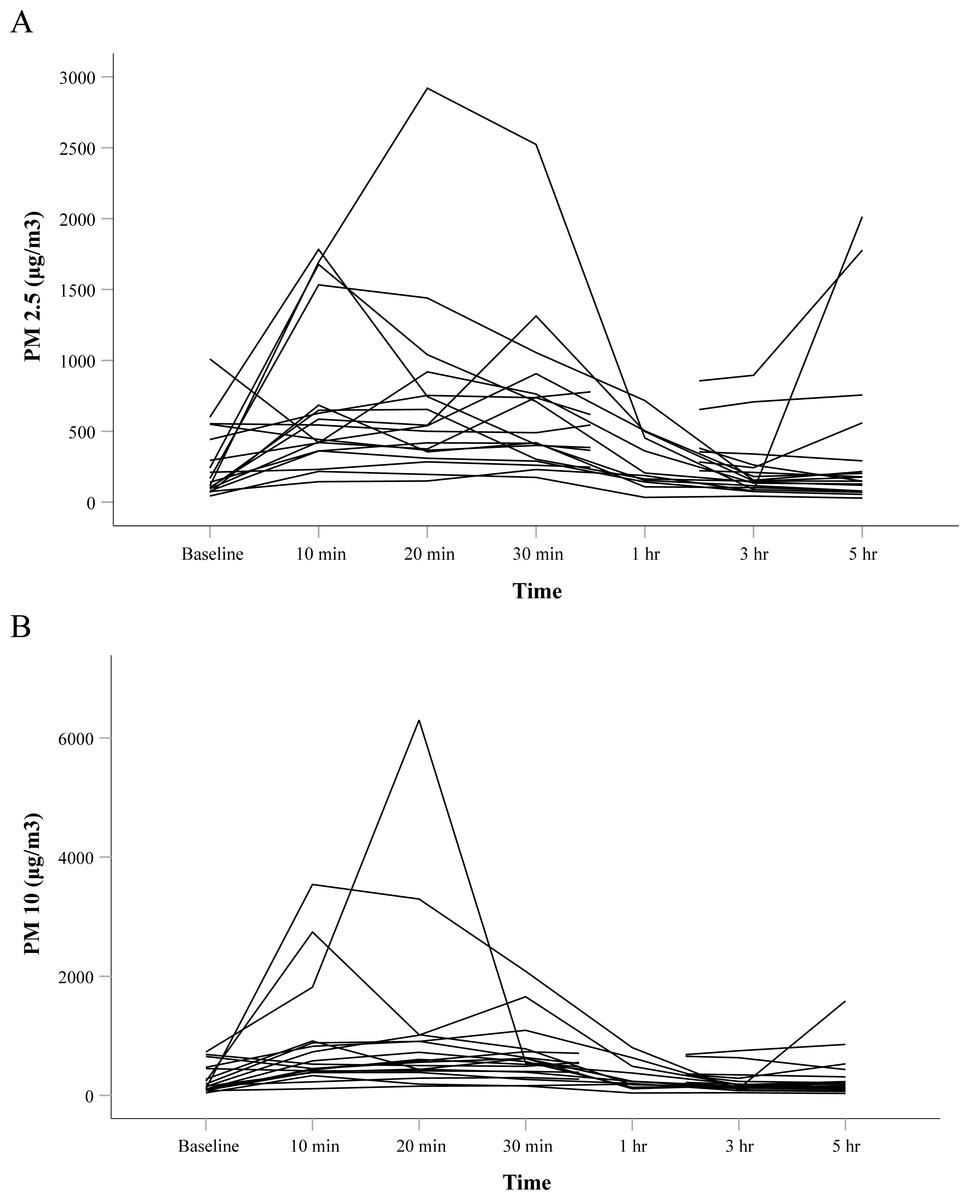
Figure 1: Spaghetti plot of (A) PM2.5 and (B) PM10 across time points.
Each line represents each participant.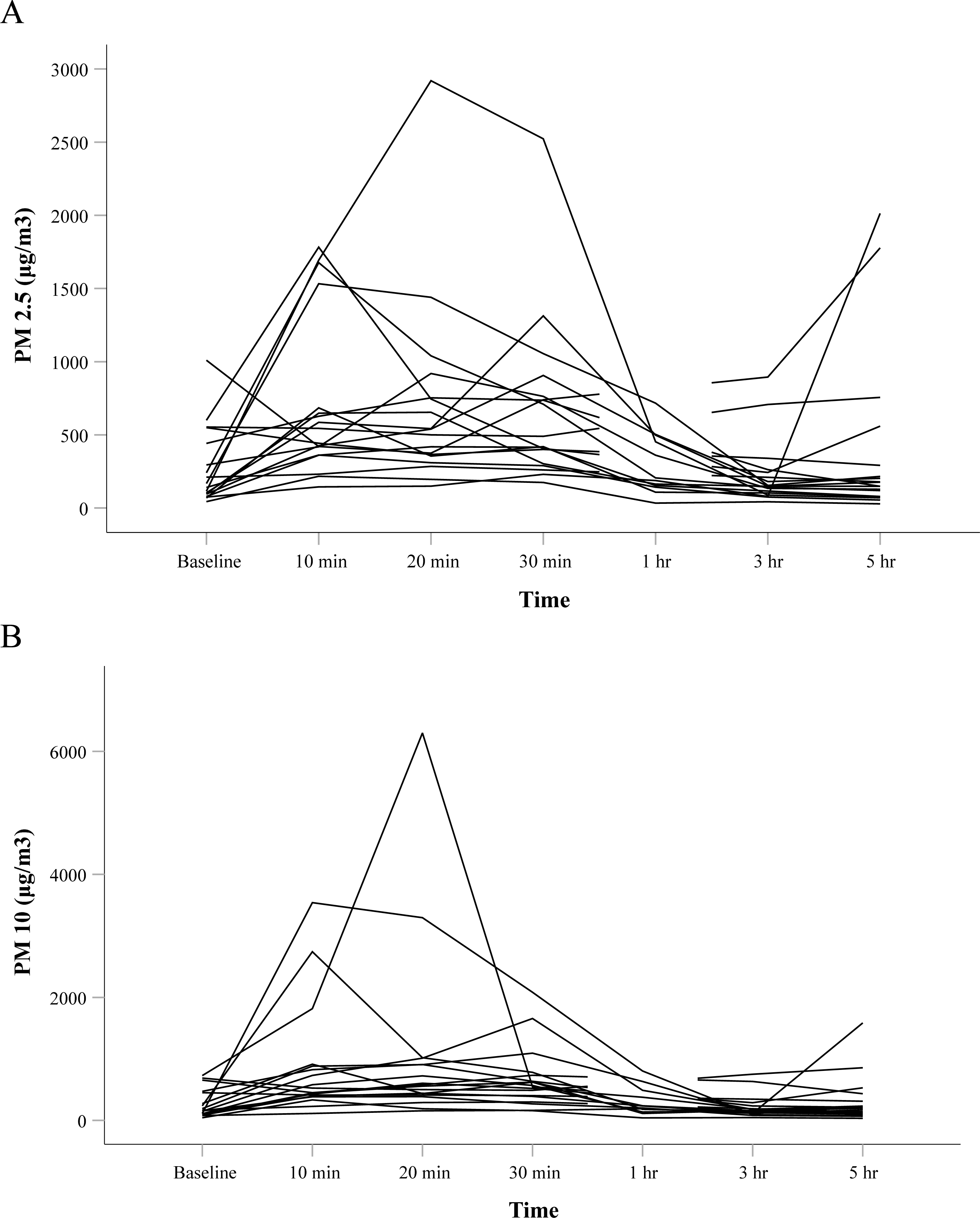{kind=link}
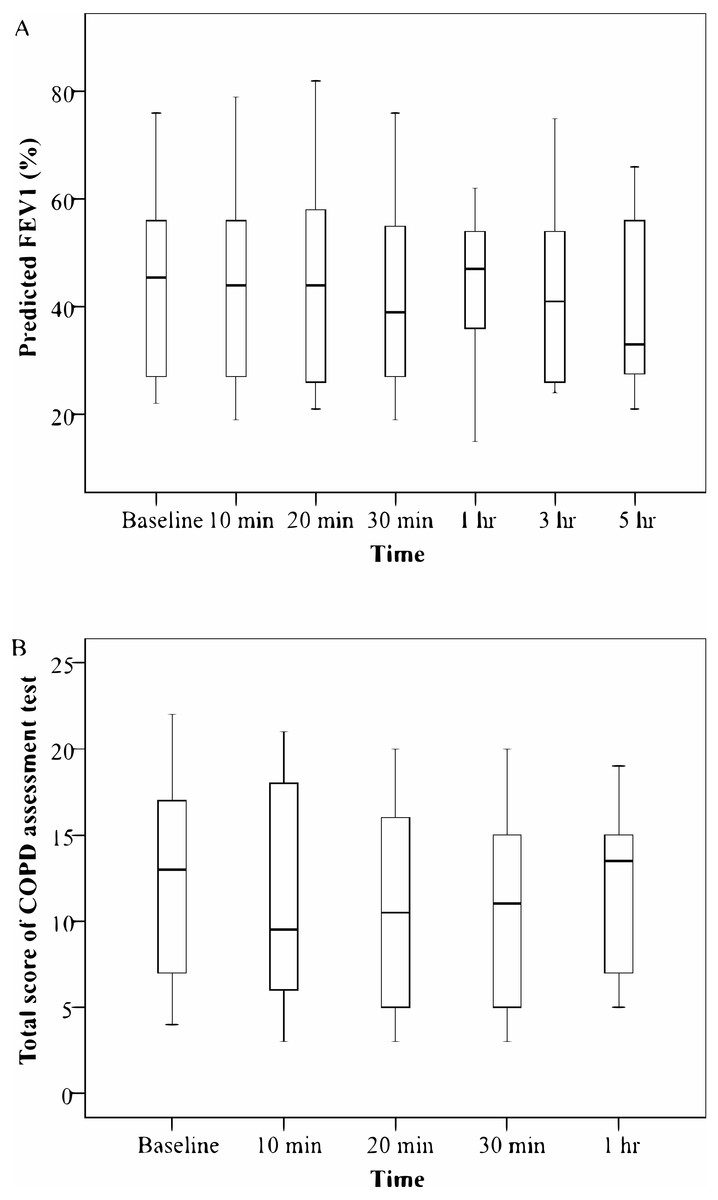
Figure 2: Box plot of (A) FEV1 predicted and (B) CAT total score across time points.
The horizontal line in the box represents the median and the box indicates the interquartile range. The asterisk “*” indicates that the values after burning inc.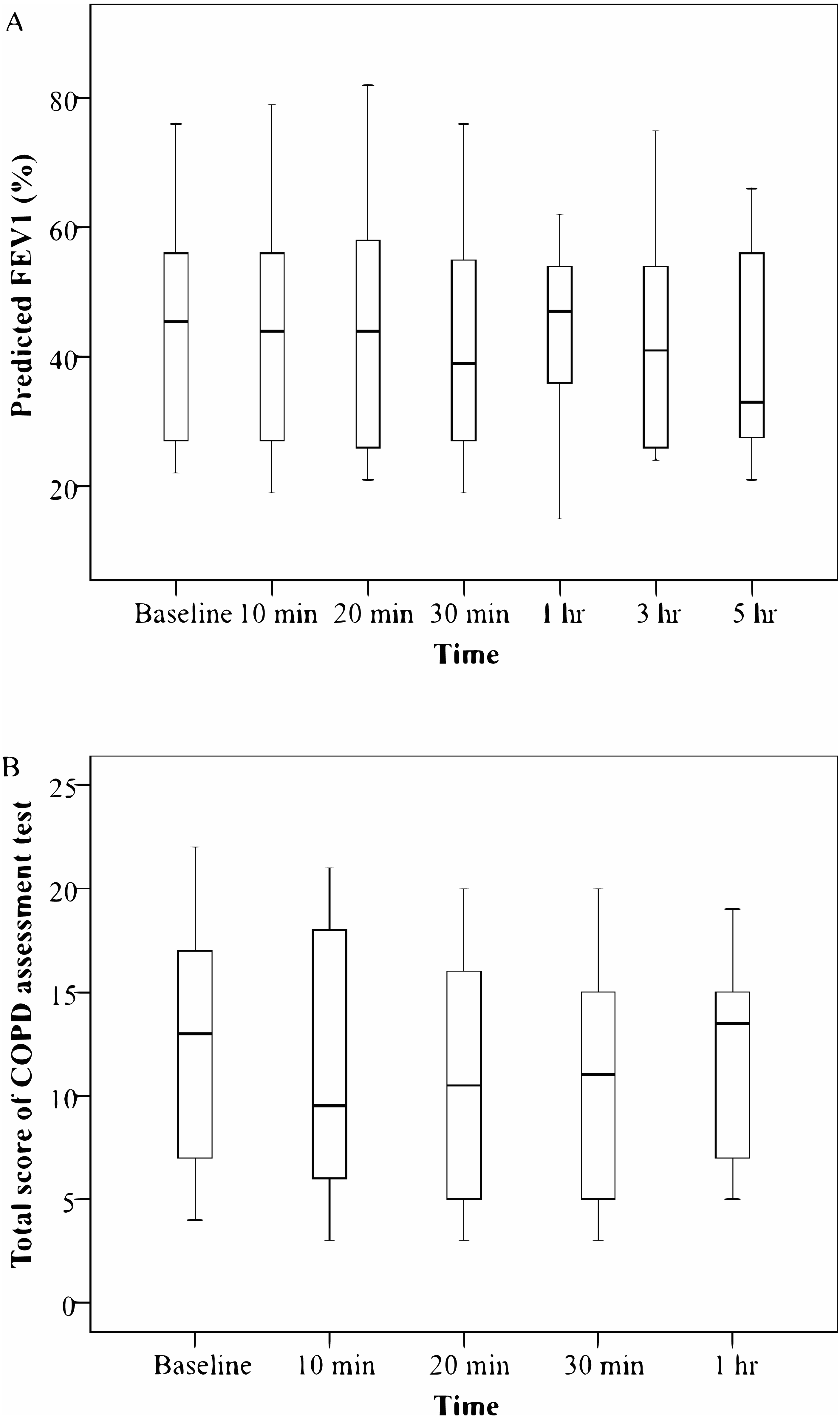{kind=link}
The effect of burning incense on PM2.5 and PM10
Figure 1 illustrates the trend of PM parameters before and after burning incense. The result of the GEE showed that the PM2.5 concentration levels significantly increased 10 min (B = 439.4, P < 0.01), 20 min (B = 423.2, P < 0.05), and 30 min (B = 439.4, P < 0.01) after burning incense, whereas the PM2.5 levels 1 h, 3 h, and 5 h after burning incense returned to baseline levels. The results concerning PM10 levels were similar to those of PM2.5, with concentration levels significantly elevated 10 min (B = 609.6, P < 0.01), 20 min (B = 774.5, P < 0.05), and 30 min (B = 403.2, P < 0.01) after burning incense, and returning to baseline levels 1 h, 3 h, and 5 h after burning incense. In addition, the corrected quasi likelihood under the independence model criterion (QICC) value for PM2.5 was 30569831 and 25604057 before and after incorporating the time effect, respectively. In contrast, the QICC value for PM10 was 72044297 and 60407238 before and after incorporating the time effect, respectively. Finally, the conclusions were not altered when changing the linking function to log and the distribution to gamma in the GEE model (data not shown).
The effect of burning incense on predicted FEV 1 and CAT scores
Figure 2 shows the trend of predicted FEV1 and CAT total scores before and after burning incense. The GEE analyses indicated that the values of both predicted FEV1 and CAT total scores did not change before and after burning incense. In addition, the QICC value for FEV1 was 31614 and 31690 before and after incorporating the time effect, respectively. In contrast, the QICC value for CAT was 2405 and 2374 before and after incorporating the time effect, respectively. At last, the conclusions were not altered when changing the linking function to log and the distribution to gamma in the GEE model (data not shown). Furthermore, there were no associations among PM10, PM2.5, and FEV1 (P > 0.05).
Discussion
Our study results showed that PM2.5 and PM10 concentration levels were highest compared to baseline levels after 30 min of incense burning, and that PM concentration levels returned to baseline levels within 1 h of incense burning. However, this finding was inconsistent with Kao & Lung’s findings (Kao & Lung, 2000). They reported that the highest PM10 level was observed 3 h after incense burning had stopped (approximately 641 ±124 µg/m3), which was an increase of over 200 µg/m3 in comparison with background concentration levels. The differences in these findings might be due to environmental factors, as Kao & Lung’s study (2000) was undertaken in a closed environment, whereas our study data were derived from a natural environment. Another possible reason for these differences may have been due to differing weather conditions.
A Taiwanese study reported that the PM2.5 level following incense burning was 9 times higher in a room with closed windows and doors than in a ventilated room (Kao & Lung, 2000). Studies undertaken in Taiwan found that PM levels were affected according to temperature, moisture, and wind speed (Chien & Chen, 2012; Tseng, 2012). In our study, it was raining on the day of the assessment for 4 participants (22.2%) whereas, for 14 participants (77.8%), it was sunny on the day of the assessment. The average humidity level inside was higher than the average humidity level outside (68.2 ± 10.3 versus 67.4 ± 10.4, respectively). Therefore, it is possible to consider our study as a field study, and that performing our study in a natural environment resulted in these lower PM concentration levels. Opened windows and doors or distancing oneself from incense burners/censers could, therefore, effectively reduce the risk of PM exposure.
Predicted FEV1 is an indicator of lung function and may indicate chronic changes in lung function (Dockery & Brunekreef, 1996); therefore, we anticipated no observable change in lung function before and after burning incense as the exposures to PM were of short duration. Considering the relationship between PM emission from incense burning and lung function, our findings were inconsistent with those of two other studies (Lin, Krishnaswamy & Chi, 2008; Chen, Ho & Yu, 2017) that reported respiratory system dysfunction or a decline in lung function were related to PM emissions from incense burning. Another study also indicated that lung function significantly decreased in patients with COPD during a period of high PM10 concentration levels (Lee et al., 2014). Through examining 2-year lung function data from 5,010 non-smoking adolescents with no respiratory-related disease, Chen, Ho & Yu (2017) reported that most of the participants had lower FVC and FEV1 levels when in an environment where the daily burning of incense occurred; nevertheless, their exposure to burning incense was not related to lung function if incense were only burned at home twice a month (Chen, Ho & Yu, 2017). Hence, the duration or frequency of incense burning is likely to be a factor influencing lung function.
The CAT score has been reported to be a reliable tool to estimate health-related conditions or to predict exacerbations among at-risk patients with COPD (Lee et al., 2014; García-Sidro et al., 2015). One study observed that CAT physical scores for patients with COPD were higher in relation to high outdoor PM2.5 concentration levels, but found that PM10 concentration levels had no relation to CAT scores (Chi et al., 2017). In contrast, another study reported that CAT scores, in terms of chest tightness and sleep disturbance, were significantly higher during high PM10 concentration level periods (Pothirat et al., 2019). However, in relation to lung function, CAT scores for patients with COPD in this study indicated no obvious changes among the participants, although the PM2.5 and PM10 emission concentration levels following incense burning were both high. This finding may be because, for CAT scores to show significant change, exposure needs to occur over a long rather than a short duration. Future studies are needed to investigate what duration of exposure is required to show changes in CAT scores and for symptoms to appear. Moreover, the CAT questionnaire results could have led to an underestimation of patients’ health conditions as the patients might have responded to the questionnaire according to their impressions of their symptoms only (Lee et al., 2014). The small sample size in this study may be another reason for our findings.
Due to the short-term exposure to incense burning, changes in lung function among patients with COPD might not have been apparent in our results. There are many possible reasons for short term exposure to PM10 or PM2.5 that do not relate to lung function. The recovery function of the lung after a short exposure is one possible reason. The total exposure time (by increasing the frequency of burnings) in a day or a month could be a good predictor. Further studies could recruit participants employed by temples and examine this relationship. The use of medication could also have been a factor influencing the inconsistent relationship between lung function and 24 h average PM concentration levels among patients (De Hartog et al., 2010), and short-term observation may be too limited to determine changes in lung function (Dockery & Brunekreef, 1996). Furthermore, short-term observations are less likely to show changes since some possible short-term effects, observable in patients whose lung function testing had been implemented within one month, for example, have been excluded from consideration to avoid influencing the outcome (Abbey et al., 1998). In contrast, long-term PM exposure has been shown to have an association with a decrease in lung function (Abbey et al., 1998; Downs et al., 2007). Therefore, if we had extended the exposure period and the follow-up period for the participants over a longer timeframe, or if we had excluded factors such as the patients’ use of medication, it is possible that our findings may have been different, and further studies are needed in this regard.
The limitations of the current study include that we only measured PM levels on one day, which only represents short-term exposure and might result in a bias in measuring human respiratory health. In addition, our study included a small sample size and only 18 COPD patients and 126 observations. The results may not be generalizable to the general COPD population, and further studies with a case control design and a large sample size are needed. Moreover, we did not analyze the composition of PM, which contains several toxic substances harmful to health. Several studies have shown that PM has many pulmonary irritants that increase lung inflammatory reactions and cytotoxicity and overall health (Kuo, Tsai & Sopajaree, 2015; Wegesser, Pinkerton & Last, 2009). Future studies should analyze the composition of PM and information on the dose of the incense burnt in households in order to examine the relationships between PM levels and the degree and trajectory of respiratory symptoms, including the dose–response association, which may provide references for nursing care and/or self-prevention within this population.
Conclusions
Our study findings showed that PM10 and PM2.5 levels were highest 30 min after incense burning and were found to be the same as background concentration levels after 1 h following incense burning. Burning incense was not found to influence lung function and respiratory symptoms in patients with COPD as the exposures to PM were of short duration. A small sample size and a short study period may have influenced these results. For future studies, a longitudinal study design with a larger sample size is recommended for examining the influence of burning incense on lung function and symptom in patients with COPD.
Supplemental Information
Questionnaires for this study
Self-reported questionnaires collected for understanding participant’s information