
Effect of short-term exposure to air pollution on ischemic stroke incidence and mortality: a five-year time-series study in Jining, China
- Published
- Accepted
- Received
- Academic Editor
- Worradorn Phairuang
- Subject Areas
- Neurology, Public Health, Environmental Health
- Keywords
- Air pollution, Ischemic stroke, Incidence, Death, Short-term exposure
- Copyright
- © 2025 Kong et al.
- Licence
- This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits using, remixing, and building upon the work non-commercially, as long as it is properly attributed. For attribution, the original author(s), title, publication source (PeerJ) and either DOI or URL of the article must be cited.
- Cite this article
- 2025. Effect of short-term exposure to air pollution on ischemic stroke incidence and mortality: a five-year time-series study in Jining, China. PeerJ 13:e20298 https://doi.org/10.7717/peerj.20298
Abstract
Background
Short-term exposure to air pollutants is associated with an increased risk of ischemic stroke incidence and mortality. However, there is a lack of research based on data from disease surveillance systems. This study used disease surveillance system data to quantitatively analyze the association between air pollution and ischemic stroke incidence and mortality in Jining, China.
Methods
The stroke registration system of the Jining City Center for Disease Control and Prevention (CDC) includes information on confirmed stroke cases reported by all medical institutions in the jurisdiction, covering a population of 8.9 million. Generalized linear regression models combined with distributed lag nonlinear models (DLNM) were used to determine the association between air pollutants and ischemic stroke incidence and mortality. Stratified analyses by sex, age, and season were also conducted.
Results
During the study period (January 1, 2018, to December 31, 2022), there were 209,949 ischemic stroke incidence cases and 23,565 ischemic stroke-related deaths. There were more ischemic stroke incidence and death cases in males compared to females. The number of incidence cases was higher in the warm season (52.6%) than in the cold season (47.4%), while this pattern was reversed for the number of deaths, with a higher number of deaths in the cold season (55.9%) than in the warm season (44.1%). This study showed that exposure to particulate matter (PM2.5 and PM10), nitrogen dioxide (NO2), and carbon monoxide (CO) was associated with ischemic stroke incidence, and exposure to PM2.5, PM10, sulfur dioxide (SO2), and CO was associated with ischemic stroke mortality. The relative risks (RRs, with 95% CIs) for ischemic stroke incidence at the maximum single-lag effect day for each interquartile range (IQR) increment for PM2.5, PM10, NO2, and CO were 1.007 (1.001–1.014), 1.004 (1.000–1.008); 1.031 (1.011–1.051), and 1.008 (1.001–1.015), respectively. The RRs (with 95% CIs) for mortality for PM2.5, PM10, SO2, and CO were 1.049 (1.025–1.073), 1.031 (1.014–1.048), 1.021 (1.001–1.041), and 1.044 (1.017–1.071), respectively. Furthermore, the association between air pollution and ischemic stroke incidence risk was modified by age and season. Individuals aged >75 years were more vulnerable to SO2-induced ischemic stroke incidence risk, and PM2.5 and CO were more harmful in the cold season.
Conclusion
These findings suggest that short-term exposure to PM2.5, PM10, SO2, NO2, and CO leads to increased ischemic stroke morbidity and mortality. The elderly population, as well as the general population, should be better protected during the cold season.
Introduction
Stroke, also known as cerebrovascular accident (CVA), has a rapid onset. In 2021, there were 11.9 million new stroke events, representing the third leading cause of deaths worldwide after ischemic heart disease and COVID-19. Ischemic stroke constituted the largest proportion of all incident strokes (7.8 million, or 65.3%), followed by intracerebral hemorrhage. Rates of incident and fatal stroke were highest for ischemic stroke (92.4 per 100,000 and 44.2 per 100,000, respectively; Collaborators, 2021). Unlike the decline in age-standardized stroke incidence and mortality in recent years in developed countries, developing countries have experienced a dramatic increase in stroke incidence and mortality due to significant population aging, with 70% of stroke incidence and 87% of stroke-related deaths occurring in low- and middle-income countries (Bell et al., 2017). Therefore, the variability of stroke risk factors should be identified among countries with different levels of economic development.
Large cohort studies have shown that, in addition to high blood pressure, smoking, and physical inactivity, air pollution is associated with stroke, and this relationship may be stronger in low- and middle-income countries (Sarker et al., 2015). The molecular mechanisms by which air pollution contributes to stroke incidence and mortality are complex, and this complexity is exacerbated by pollutant interactions. In previous studies, air pollutants, including particulate matter pollutants (PMx), sulfur dioxide (SO2), carbon monoxide (CO), and nitrogen dioxide (NO2), have been shown to affect stroke incidence, prognosis, and death by causing oxidative stress and systemic inflammatory responses, promoting atherosclerosis formation, damaging vascular endothelial cells, increasing blood viscosity and thrombosis, and causing cardiac arrhythmias and elevated blood pressure (Bobb et al., 2015; Liang et al., 2014; Nemmar et al., 2011; Thomson et al., 2007).
Current epidemiologic studies of the association between air pollution and stroke are deficient, resulting in large discrepancies or even conflicting conclusions (Baum et al., 2017; Butland et al., 2017; Mecocci et al., 2018; Wellenius & Joel Schwartz, 2005). Using stroke admissions as the outcome of interest may be biased because people may not go to the hospital on the same day they experience symptoms or discomfort, and there may be a delay between stroke onset and admission. In addition, due to potential selection bias, admission data may not fully reflect the true incidence of the disease in the local population (Ban et al., 2021; Chen et al., 2022). Registry datasets covering all stroke case records from multiple sources may be relatively reliable in reflecting local stroke incidence because of decreased misclassification of disease and improved completeness; however, to date, there have been few studies based on population-based registry data (Butland et al., 2017). In addition, racial stratification, geographic differences, and varying levels of pollution due to differences in industrial infrastructure all contribute to the wide variation in study results (Chen et al., 2014; Scheers et al., 2015; Wang, Liu & Li, 2016).
Understanding the relationship between air pollution and ischemic stroke is crucial for public health policymaking and the development of effective intervention strategies aimed at reducing the burden of stroke. In this context, the current epidemiologic study used population-based registry data from the disease surveillance system in a highly polluted area with a robust coal industry to examine the association between short-term exposure to air pollutants and stroke incidence and mortality and to explore the potential effects of gender, age, and season.
Materials & Methods
Study area and data collection
Jining is located in the southwest of Shandong Province, East China, covering an area of 11,100 km2 with a permanent population of 8.9 million in 2022. The coal-containing area of Jining exceeds 3,920 km2, accounting for more than 1/3 of the total land area of the city, and is one of the eight major coal-based cities in China. Coal and its derivative industries have introduced substantial pollution to the environment of Jining. Although the government has taken active measures to combat air pollution in recent years, the air quality of Jining still ranked second to last in Shandong Province in 2022 (Chiu et al., 2023).
Daily ischemic stroke incidence data were sourced from the stroke registration system of the Jining Centers for Disease Control and Prevention (CDC). This system requires all medical facilities including hospitals, clinics, and community health centers within the jurisdiction to provide timely reports on cases diagnosed as stroke. Stroke deaths that did not involve hospitalization were also included. The registration data includes basic patient information, clinical symptoms, and medical examination results that are categorized according to the International Classification of Diseases version 10 (ICD-10). The date of the occurrence of clinical symptoms is recorded as the incidence date. The time frame of this study was from January 1, 2018 to December 31, 2022, and the study population consisted of all ischemic stroke (ICD code: I63) cases recorded in the system. The private information of patients, such as name, ID number, and medical insurance number, was not collected during data export.
Environmental data and exposure assessment
Air pollution data including PM2.5, PM10, SO2, NO2, and CO were obtained from the China Air Quality Online Monitoring and Analysis Platform or the National Urban Air Quality Real-time Publishing Platform, covering six air quality monitoring stations in Jining City (http://www.cnemc.cn/sssj/). Data measurements were in accordance with Chinese National Quality Control (GB3095-2012) protocols. The 24-hour average concentration of a pollutant was used to represent the daily exposure level for each individual. Daily mean temperature was sourced from the National Meteorological Information Center of China. Single-day lag exposures and cumulative lag effects were calculated. For example, the effect at lag 0–1 day was defined as the single-day lagged effect for the lag 0 day and lag 1 day. The effect at lag 02 day was defined as the cumulative lagged effect of lag 0, lag 1, and lag 2 days. The effect at lag 01–02 was defined as the effect at the lag 01 and lag 02 days.
Statistical analysis
Daily ischemic stroke incidence and mortality, concentration of air pollutants, and temperature were established as time series and expressed as maximum (Max), minimum (Min), median (Median), mean (Mean), standard deviation (SD), and interquartile range (IQR). Spearman’s correlation coefficient was used to estimate the relationship between pollutants and temperature. The effects of air pollutants on ischemic stroke are lagged and nonlinear, and distributed lag nonlinear models (DLNMs) were used to estimate the exposure-lag effect of short-term air pollution exposure on ischemic stroke incidence and mortality (Ban et al., 2021; Gasparrini, Armstrong & Kenward, 2010). Since the daily ischemic stroke incidence and death data are quantitative data and are small probability events, the DLNM combined with a quasi-Poisson regression model was applied. The model is as follows:
where Yt is the expected value of incidence or mortality on day t; α is the intercept term; cb is the cross-basis function; pollutant is air pollution, and Mean Tempt is mean temperature. There is often a lagged effect between air temperature and health outcomes, so the parameter settings used in this study for temperature confounding control were consistent with those for pollutants, using both linear and natural cubic spline fits to the lag-response relationship and the respective association with the ending exposure-response relationships, with degrees of freedom (df) set to 3. The nonlinear relationship between air pollution and ischemic stroke was explored through a natural cubic spline function (df = 3) when the cumulative effect appeared to be strongest. The variable ns (time, df = 7*years) represents a degree of freedom of 7 per year for controlling for long term trends and seasonality. DOW denotes the day of the week, and holiday denotes the effect of the holiday that both variables were included as dummy variables.
Studies have shown that the duration of cardiovascular effects of air pollution generally lasts 1–5 days. To fully examine the lag effect, the maximum number of lag days in the crossbasis was set at 7 days in this study. A single-pollutant model was used to assess the association between air pollution and ischemic stroke incidence or mortality to avoid air pollutant correlation. The risk estimates for air pollutants were expressed as relative risks (RRs) with their 95% confidence intervals (CIs) in ischemic stroke incidence and mortality when the concentration of each air pollutant increases by per interquartile range (IQR).
Effect modification
Stratified analyses by age (≤75 years, >75 years), sex (male, female), and season (cold season, October to March; warm season, April to September) were performed to explore potential effect modifiers of associations. A subsequent z test was performed to determine whether significant differences existed between subgroups (Altman & Bland, 2003; Liu et al., 2021).
Sensitivity analysis
The robustness of the results was determined in the sensitivity analysis by fitting a two-pollutant model (incorporating pollutants with correlation coefficients <0.6 to avoid covariance), varying the degrees of freedom of the natural cubic spline function for time (df = 6–8) and temperature (df = 4–6). All analyses were conducted through R (version 4.3.1, R Institute for Statistical Computing, Vienna, Austria) and related packages like “dlnm” and “splines”. A two-sided P-value < 0.05 was considered statistically significant.
Ethical approval
This study was approved by the Ethics Committee of the Jining Center for Disease Control and Prevention. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research/review board (IRB)-IRB Number: (2024-005). Study participation only required verbal informed consent, which was obtained from all subjects who participated in this study and was approved by the ethics committee.
Results
Population and exposure characteristics
During the study period (January 1, 2018 to December 31, 2022), there were 209,949 ischemic stroke incidence cases and 23,565 ischemic stroke-related death cases. There were more ischemic stroke incidence and death cases in males than in females. The number of incidence cases was higher in the warm season (52.6%) than in the cold season (47.4%), while this pattern was reversed for the number of deaths, with a higher number in the cold season (55.9%) than in the warm season (44.1%). During the study period, the daily mean (with maximum) values of PM2.5, PM10, SO2, CO, NO2, and temperature were 50.6 (241.1) µg/m3, 89.3 (1017.1) µg/m3, 31.1 (108.3) µg/m3, 0.9 (2.8) mg/m3, 14.1 (49.8) µg/m3 and 16.8 (36.2) °C, respectively. Detailed information is presented in Table 1. The concentrations of each air pollutant (including PM2.5, PM10, SO2, CO, and NO2) showed obvious cyclical changes during the study period, with high concentrations in the cold season and low concentrations in the warm season, consistent with the changes in atmospheric dispersion conditions and pollutant sources (Fig. S1). The SO2 concentration peaked in 2018 and began to gradually decrease, due to the strict control of industrial pollution sources in Jining, especially the upgrading of desulfurization measures related to the coal burning industry. There were positive correlations between PM2.5, PM10, NO2, CO, and SO2 (Pearson’s r range: 0.39–0.77; PM2.5 was strongly correlated with PM10 and CO, Pearson’s r > 0.7) and all pollutants showed negative correlations with temperature. (Table 2).
| Variables | Mean ± SD | Min | P25 | P50 | P75 | P95 | Max | ||
|---|---|---|---|---|---|---|---|---|---|
| Air pollutants | |||||||||
| PM2.5 (μg/m3) | 50.6 ± 34.2 | 3.7 | 27.7 | 40.8 | 62.4 | 123.9 | 241.1 | ||
| PM10 (μg/m3) | 89.3 ± 57.8 | 8.7 | 55.2 | 76.5 | 108.5 | 180.8 | 1,017.1 | ||
| SO2 (μg/m3) | 31.1 ± 16.2 | 4.7 | 18.5 | 26.8 | 42.0 | 62.2 | 108.3 | ||
| CO (mg/m3) | 0.9 ± 0.3 | 0.2 | 0.7 | 0.8 | 1.0 | 1.4 | 2.8 | ||
| NO2 (μg/m3) | 14.1 ± 6.9 | 2.4 | 9.3 | 12.5 | 17.5 | 27.6 | 49.8 | ||
| Meteorological factor | |||||||||
| Temperature (°C) | 16.8 ± 9.8 | −7.49 | 8.4 | 17.3 | 25.7 | 30.3 | 36.2 | ||
| Ischemic stroke cases | |||||||||
| Total | |||||||||
| Incidence | 209,949 | 114.98 ± 32.34 | 34.0 | 92.0 | 114.0 | 135.0 | 168.0 | 338.0 | |
| Death | 23,565 | 12.91 ± 8.03 | 1 | 8.0 | 12.0 | 17.0 | 25.0 | 180.0 | |
| Sex | |||||||||
| Male | Incidence | 120,264 | 65.86 ± 19.65 | 16.0 | 52.0 | 64.0 | 78.0 | 99.0 | 211.0 |
| Death | 13,549 | 7.42 ± 5.13 | 0 | 4.0 | 7.0 | 10.0 | 15.0 | 110.0 | |
| Female | Incidence | 89,685 | 49.12 ± 14.76 | 13.0 | 39.0 | 49.0 | 58.0 | 75.0 | 141.0 |
| Death | 10,016 | 5.49 ± 3.83 | 0 | 3.0 | 5.0 | 7.0 | 12.0 | 70.0 | |
| Age | |||||||||
| ≤75 | Incidence | 148,558 | 81.36 ± 23.47 | 22.0 | 65.0 | 80.0 | 95.0 | 119.0 | 247.0 |
| Death | 9,937 | 5.44 ± 4.22 | 0 | 3.0 | 5.0 | 7.0 | 12.0 | 108.0 | |
| >75 | Incidence | 61,391 | 33.62 ± 10.87 | 9.0 | 26.0 | 33.0 | 40.0 | 51.7 | 100.0 |
| Death | 13,628 | 7.46 ± 4.92 | 0 | 4.0 | 7.0 | 10.0 | 15.0 | 72.0 | |
| Season | |||||||||
| Warm | Incidence | 110,515 | 120.78 ± 32.65 | 34.0 | 98.0 | 119.0 | 140.0 | 172.0 | 325.0 |
| Death | 10,401 | 11.37 ± 5.77 | 0 | 7.0 | 11.0 | 15.0 | 22.2 | 35.0 | |
| Cold | Incidence | 99,434 | 109.15 ± 30.96 | 44.0 | 87.0 | 106.0 | 127.0 | 164.0 | 338.0 |
| Death | 13,164 | 14.45 ± 9.55 | 1 | 9.0 | 13.0 | 19.0 | 27.0 | 180.0 | |
| Variables | PM2.5 | PM10 | NO2 | CO | SO2 | Temperature |
|---|---|---|---|---|---|---|
| PM2.5 | 1.00 | |||||
| PM10 | 0.75** | 1.00 | ||||
| NO2 | 0.66** | 0.52** | 1.00 | |||
| CO | 0.77** | 0.57** | 0.58** | 1.00 | ||
| SO2 | 0.39** | 0.40** | 0.54** | 0.39** | 1.00 | |
| Temperature | −0.51** | −0.36** | −0.55** | −0.29** | −0.34** | 1.00 |
Notes:
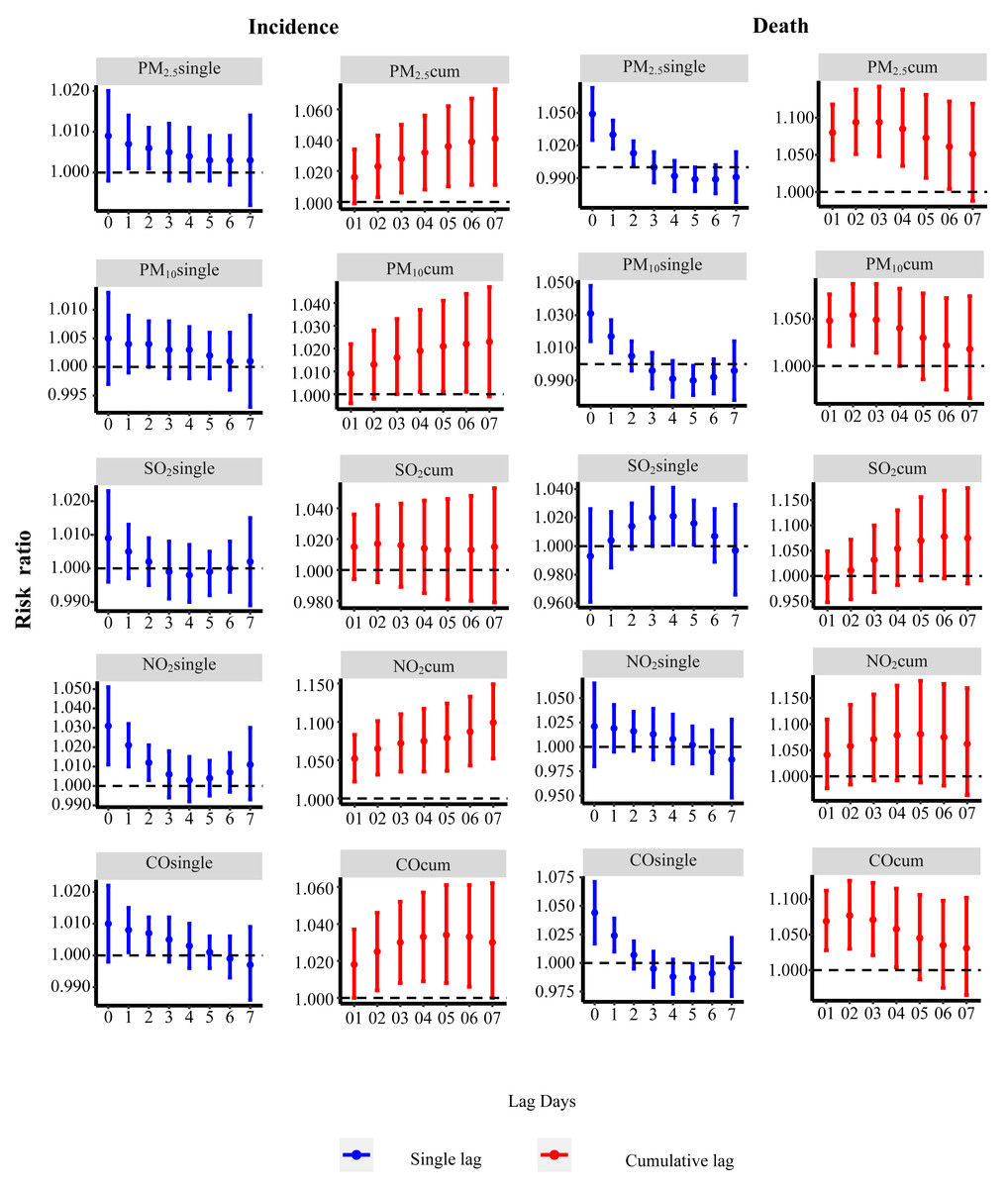
Figure 1: Relative risk of ischemic stroke incidence or death associated with air pollution in a single or cumulative lag day structure.
RRs and 95% CIs were calculated for each IQR increment.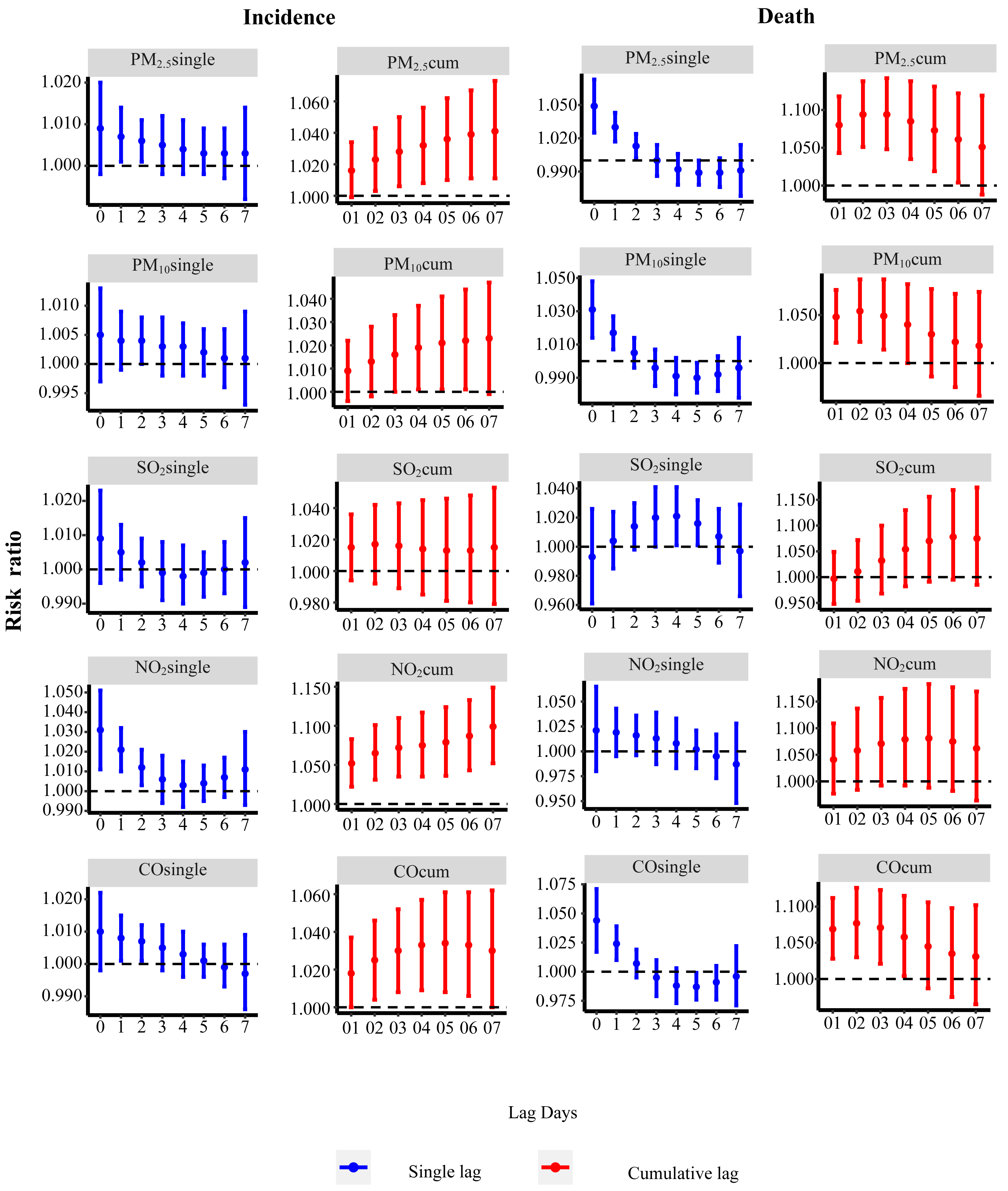{kind=link}
Association between air pollution and ischemic stroke incidence and mortality
In the single-day pollutant model (Fig. 1), after adjusting for the effect of temperature, the single-day lagged structures showed that exposure to PM2.5 (at lag 2–3 day), PM10 (at lag 3 day), NO2 (at lag 0-3 day), and CO (at lag 2–3 day) was associated with ischemic stroke incidence, and PM2.5 (at lag 0–2 day), PM10 (at lag 0–1 day), SO2 (at lag 3–5 day), and CO (at lag 0–1 day) were associated with ischemic stroke mortality. The RRs (with 95% CIs) for ischemic stroke incidence at the maximum single-lag effect day for each IQR increment for PM2.5, PM10, NO2, and CO were 1.007 (1.001–1.014), 1.004 (1.000–1.008), 1.031 (1.011–1.051), and 1.008 (1.001–1.015), respectively; the RRs (with 95% CIs) for mortality for PM2.5, PM10, SO2, and CO were 1.049 (1.025–1.073), 1.031 (1.014–1.048), 1.021 (1.001–1.041), and 1.044 (1.017–1.071), respectively. Cumulative lagged structures showed that exposure to PM2.5 (at lag02–07 day), PM10 (at lag03–06 day), NO2 (at lag01–07 day), and CO (at lag02-06 day) was associated with ischemic stroke incidence, and that PM2.5 (lag01–06 day), PM10 (lag 01–03 day), and CO (lag 01–04 day) were associated with ischemic stroke mortality. The RRs (95% CIs) of ischemic stroke incidence at the maximum cumulative-lag effect day for each IQR increment in air pollutant concentration for PM2.5, PM10, NO2, and CO were 1.041 (1.011–1.073), 1.022 (1.001–1.044), 1.099 (1.052–1.149), and 1.034 (1.008–1.061), respectively; the RRs (95% CIs) of mortality for PM2.5, PM10, and CO were 1.094 (1.051–1.138), 1.054 (1.022–1.087), and 1.077 (1.030–1.126), respectively.
Subgroup analyses of the association between air pollution and ischemic stroke incidence or mortality
The association between air pollution and the incidence or mortality of ischemic stroke was investigated through subgroup analysis based on sex, age, and season of incidence time, to determine the potential modifying effects of these variables.
Figures 2 and 3 illustrate a positive association between the risk of ischemic stroke incidence and NO2 that was observed in both male and female subgroups, as well as between stroke incidence and PM2.5in the male subgroup. The >75-year-old subgroup and ≤75-year-old subgroup showed positive associations between NO2 (at lag0–2) and, similarly, exposure to SO2 showed a positive association with the incidence of ischemic stroke in the >75-year-old group (lag03, lag04, lag05, lag06, lag07), while no association was observed in the ≤75-year-old group, indicating a modification effect of age (all P < 0.05). Subgroup analysis based on the season of incidence showed a positive association between the risk of ischemic stroke incidence and NO2 at lag0–2 in the cold season and lag6–7 in the warm season. In addition, the risk of ischemic stroke incidence showed a positive association with PM2.5 at lag1 in the cold season and with CO at lag1 in the warm season. Furthermore, the season of incidence showed modification effects, with the population being more sensitive to exposure to PM2.5(lag1, lag02, lag03, lag04) and CO (lag1, lag02, lag03) in the cold season (all P < 0.05). For ischemic stroke mortality, results were similar to the above findings (Figs. S2–S3); however, sex, age, and season of mortality did not show a modifying effect.
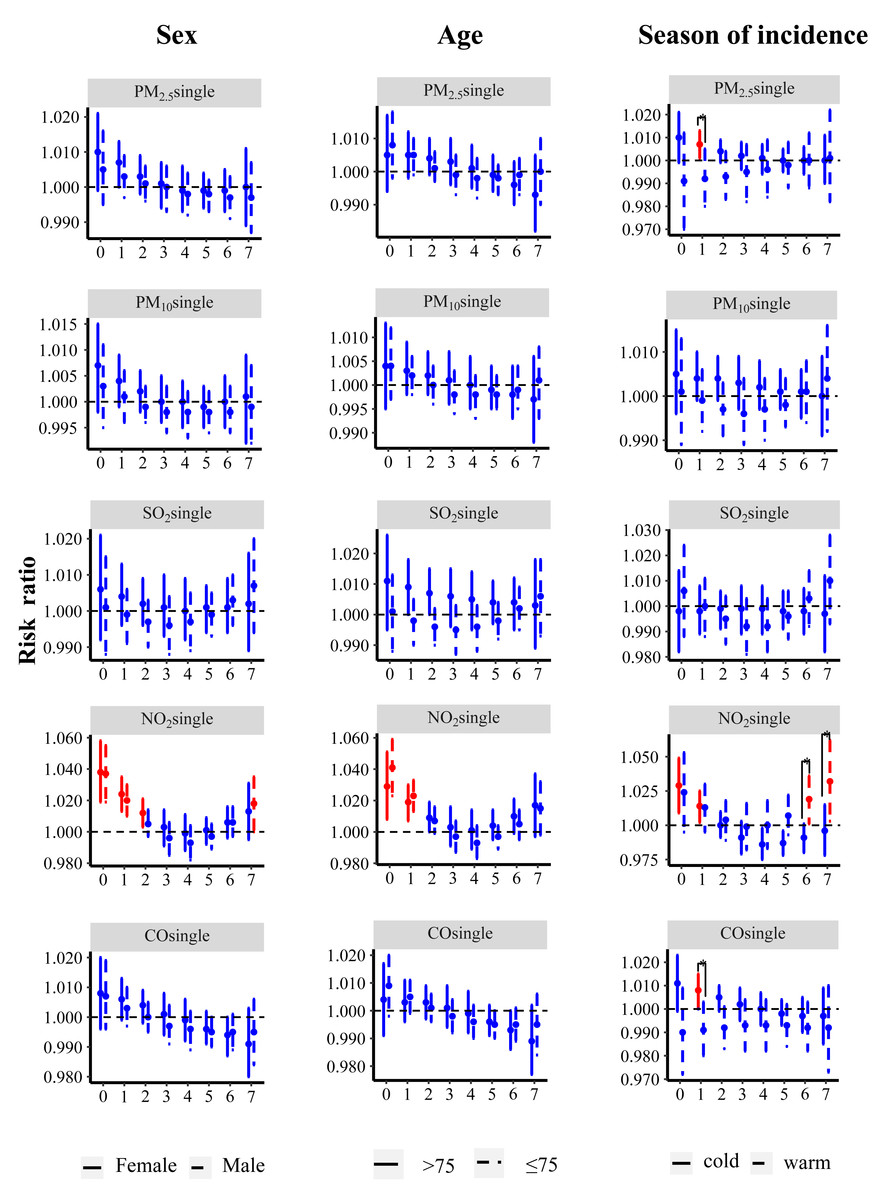
Figure 2: Relative risk of ischemic stroke incidence associated with air pollution exposure stratified by sex, age, and season of incidence in a single lag day structure.
Red color indicates the association was significant. * Indicates significant difference between two subgroups. RRs and 95% CIs were calculated for each IQR increment.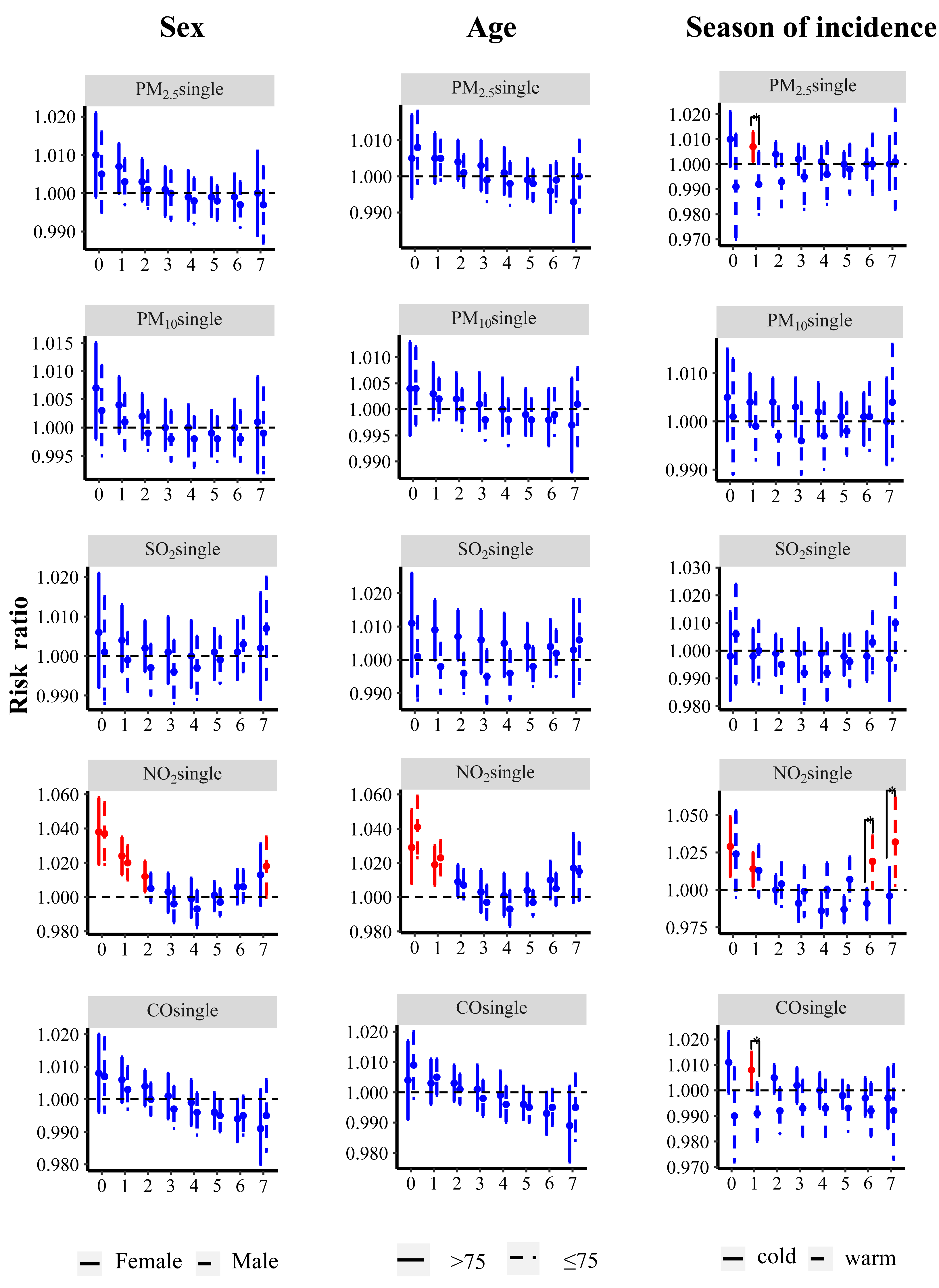{kind=link}
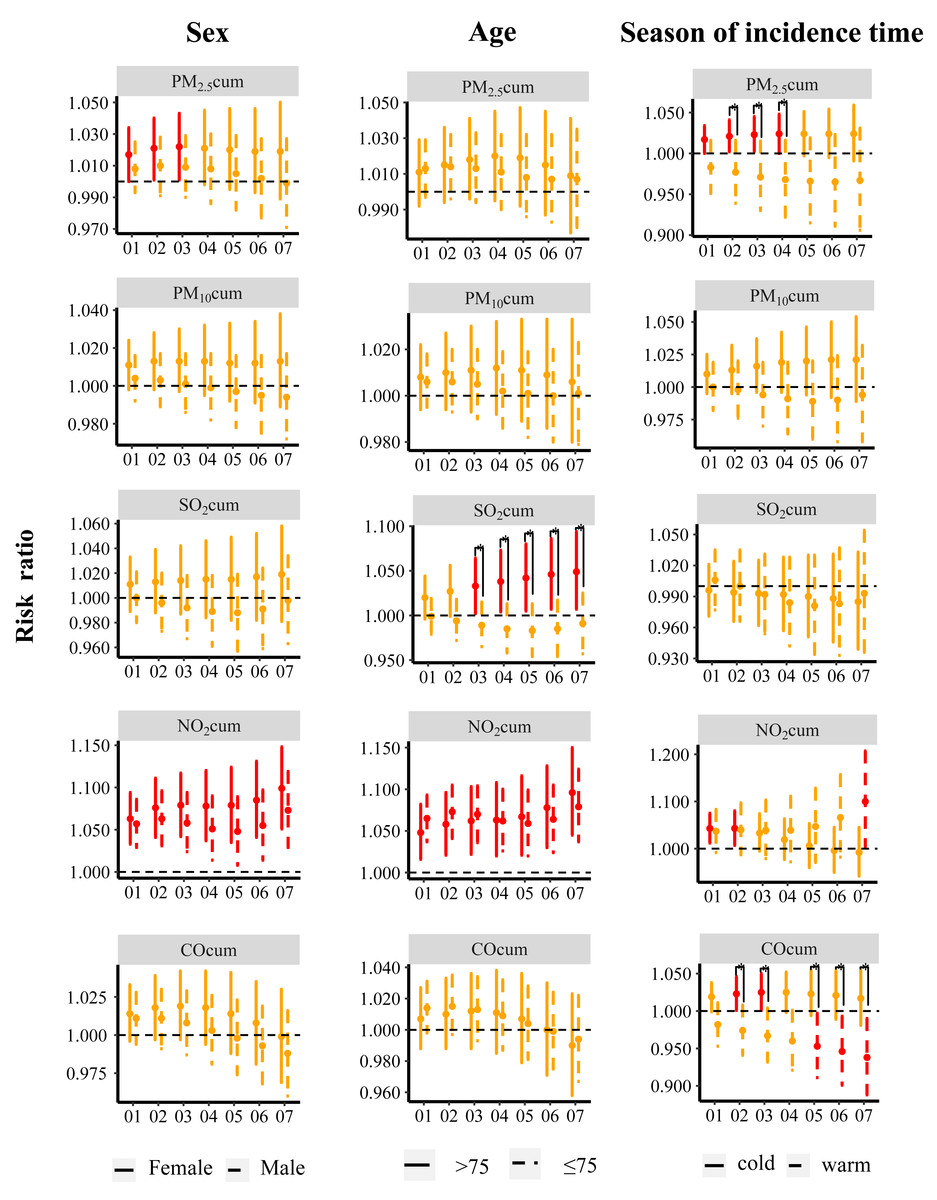
Figure 3: Relative risk of ischemic stroke incidence associated with air pollution exposure stratified by sex, age, and season of incidence in a cumulative day structure.
Red color indicates the association was significant. * Indicates a significant difference between two subgroups. RRs and 95% CIs were calculated for each IQR increment.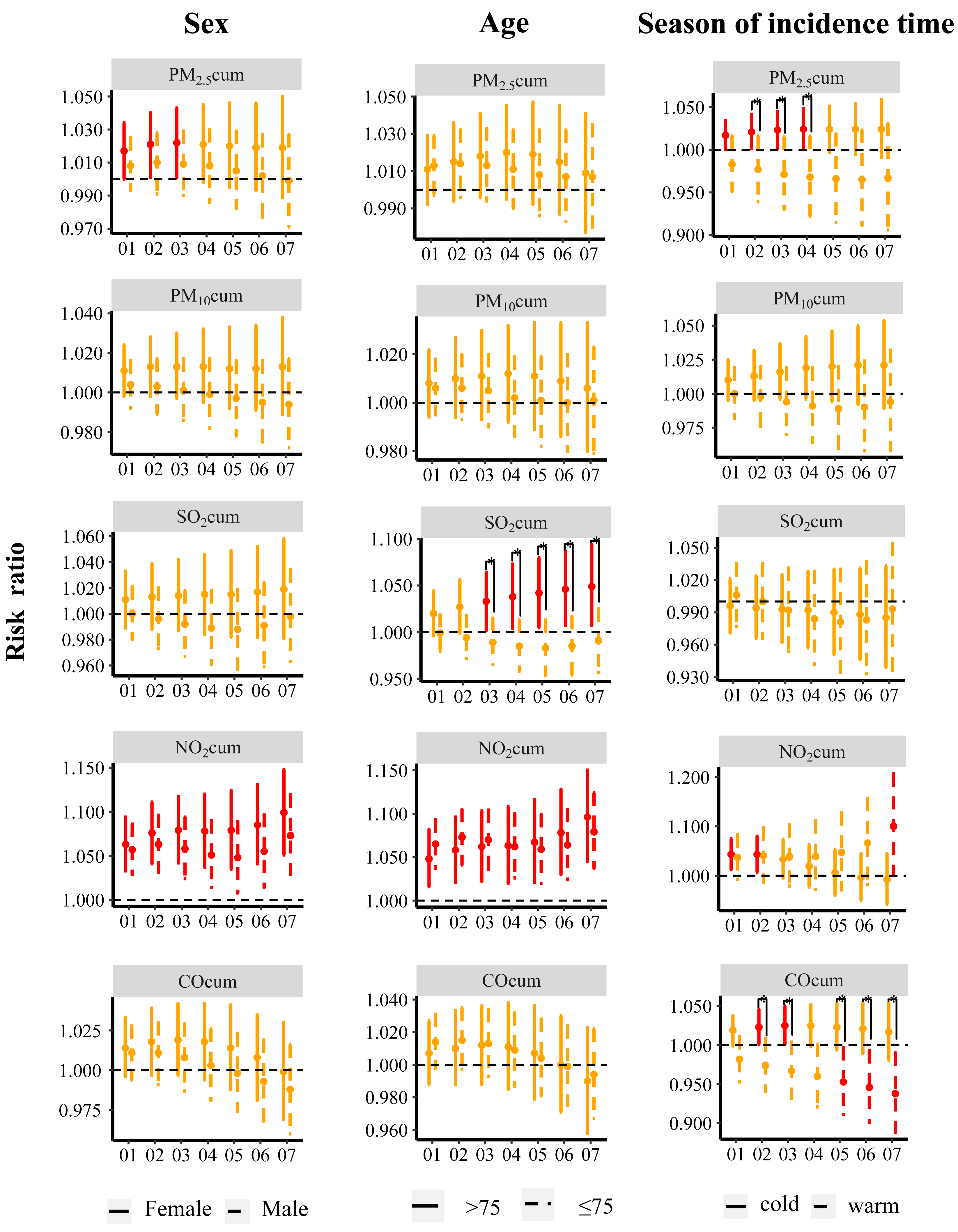{kind=link}
Sensitivity analyses
The results of the sensitivity analysis are presented in Tables 3 and 4. Using the same pollutant exposure and ischemic stroke incidence and mortality data, a two-pollutant model was constructed. After adjusting for exposure to other pollutants, there was no significant change in the association between the individual pollutants and ischemic stroke incidence or mortality (Table 3). Changing the df value did not have a substantial impact on the association between air pollutant and ischemic stroke incidence or mortality (Table 4).
| RR (95% CI)a | P value | RR (95% CI)b | P value | ||
|---|---|---|---|---|---|
| PM2.5 | null | 1.041 (1.011–1.073) | 1.094 (1.051–1.138) | ||
| SO2 | 1.043 (1.011–1.075) | 0.952 | 1.094 (1.050–1.139) | 0.990 | |
| NO2 | 1.015 (0.981–1.050) | 0.575 | 1.101 (1.052–1.152) | 0.847 | |
| PM10 | null | 1.022 (1.001–1.044) | 1.054 (1.022–1.087) | ||
| SO2 | 1.021 (0.999–1.044) | 0.962 | 1.054 (1.022–1.088) | 0.979 | |
| NO2 | 1.002 (0.978–1.026) | 0.224 | 1.048 (1.014–1.084) | 0.818 | |
| CO | 1.014 (0.990–1.039) | 0.625 | 1.041 (1.006–1.077) | 0.596 | |
| NO2 | null | 1.099 (1.052–1.149) | 1.081 (0.988–1.183) | ||
| CO | 1.105 (1.048–1.164) | 0.891 | 1.039 (0.931–1.159) | 0.582 | |
| SO2 | 1.116 (1.061–1.173) | 0.661 | 1.059 (0.958–1.171) | 0.768 | |
| CO | null | 1.034 (1.008–1.061) | 1.077 (1.030–1.126) | ||
| SO2 | 1.035 (1.008–1.062) | 0.970 | 1.079 (1.031–1.129) | 0.963 |
| df | PM25 | PM10 | SO2 | NO2 | CO | ||
|---|---|---|---|---|---|---|---|
| Incidence | time | 6 | 1.047 (1.016–1.078) | 1.021 (1.000–1.043) | 1.015 (0.990–1.040) | 1.107 (1.060–1.155) | 1.034 (1.009–1.061) |
| 8 | 1.037 (1.007–1.068) | 1.022 (1.001–1.044) | 1.013 (0.988–1.037) | 1.092 (1.044–1.143) | 1.029 (1.003–1.056) | ||
| 9 | 1.035 (1.004–1.066) | 1.021 (1.000–1.043) | 1.016 (0.990–1.042) | 1.085 (1.035–1.136) | 1.028 (1.002–1.054) | ||
| T | 4 | 1.037 (1.007–1.068) | 1.021 (1.000–1.043) | 1.009 (0.984–1.033) | 1.082 (1.036–1.131) | 1.036 (1.011–1.063) | |
| 5 | 1.046 (1.015–1.077) | 1.023 (1.002–1.045) | 1.006 (0.982–1.031) | 1.085 (1.039–1.134) | 1.042 (1.016–1.069) | ||
| 6 | 1.040 (1.009–1.073) | 1.023 (1.001–1.045) | 1.006 (0.981–1.030) | 1.079 (1.033–1.128) | 1.039 (1.013–1.066) | ||
| Death | time | 6 | 1.096 (1.053–1.140) | 1.054 (1.022–1.086) | 1.021 (1.001–1.041) | 1.075 (0.984–1.175) | 1.079 (1.033–1.128) |
| 8 | 1.091 (1.049–1.136) | 1.054 (1.021–1.087) | 1.022 (1.002–1.042) | 1.090 (0.994–1.195) | 1.074 (1.027–1.123) | ||
| 9 | 1.089 (1.046–1.133) | 1.054 (1.022–1.087) | 1.022 (1.002–1.042) | 1.091 (0.993–1.199) | 1.073 (1.026–1.123) | ||
| T | 4 | 1.089 (1.046–1.133) | 1.050 (1.018–1.083) | 1.021 (1.001–1.041) | 1.072 (0.98–1.1730) | 1.071 (1.024–1.120) | |
| 5 | 1.090 (1.047–1.134) | 1.051 (1.019–1.084) | 1.022 (1.002–1.042) | 1.076 (0.983–1.177) | 1.071 (1.024–1.121) | ||
| 6 | 1.086 (1.043–1.130) | 1.052 (1.019–1.085) | 1.022 (1.002–1.043) | 1.074 (0.982–1.175) | 1.069 (1.022–1.118) |
Discussion
Air pollution causes serious health problems and economic burdens globally, with many studies linking it to cardiovascular and respiratory diseases, among others. Research on the association between stroke and air pollution continues to intensify. Ischemic stroke is the most common stroke subtype and is characterized by arterial blockage leading to reduced blood flow to brain tissue. This time-series study investigated the association between multiple air pollutants and ischemic stroke in a total of 209,949 patients with ischemic stroke incidence and 23,565 patients with ischemic stroke death between 2018 and 2022. This study found that air pollutants contribute to ischemic stroke incidence and mortality, while age, sex, and season of exposure can influence the effect of pollutants.
In this study, PM2.5, PM10, SO2, and CO were associated with ischemic stroke mortality. This is consistent with previous studies. Hu et al. (2018) reported that for every 10 µg/m3 increment in PM2.5 and PM10 concentrations on days lag0–2, the risk of stroke mortality in the exposed population increased by 0.72% and 0.68%, respectively. Similarly, in another study in southeast Chengdu, for every one unit increment in PM2.5 and PM10 exposure, the risk of stroke mortality for days lag0–10 increased by 0.25 and 0.14, respectively (Luo et al., 2019). Long-term exposure to air pollutants can also lead to similar results, with a prospective cohort trajectory analysis showing that for long-term exposure to PM2.5, the hazard ratios for direct transition from health to mortality for each five µg/m3 increment in pollutant concentration were 1.30 (1.21, 1.40); (Tian et al., 2022). Using mortality data as an outcome underestimates the impact of environmental pollution on stroke. Deaths due to acute stroke episodes tend to occur rapidly, and some patients are not included in the stroke death population because the diagnostic process stops at the prehospital emergency stage, prior to systematic imaging and laboratory diagnosis. Thus, hospitalization rates better reflect the impact of air pollutants on exposed populations than mortality rate. In a study based on data from three hospitals in Chongqing, it was shown that for each IQR increment increase in the concentrations of PM2.5, PM10, and SO2, the hospitalization rate of ischemic stroke increased by 1.2%, 1.0% and 4.8%, respectively (Chen et al., 2022). In contrast, another study based on a population in the coastal Beibu Gulf region of China did not show significant associations between PM1 or PM2.5 and stroke hospitalization rates (Chen et al., 2022; Li et al., 2023). Similar to the Beibu Gulf region of China, Ireland has relatively low levels of air pollution, and a study in Ireland by Byrne et al. (2020) showed no significant association between stroke admissions and any individual air pollutant. Excluding differences in study design (case-crossover or time-series) and air pollutant concentration levels, the use of hospitalization data may still produce unpredictable bias. There is a time lag between the onset of symptoms and hospitalization, and this lag is influenced by the level of economic development of the region. Healthcare performance of stroke patients varies by socioeconomic status (Kim et al., 2021; Li et al., 2023). The government-led disease surveillance and registry system covers all levels of hospitals and community health centers. Compared with collecting admission data from selected hospitals, this system accounts for people of different income levels, and the data collection is more robust. In the current study, population-based disease surveillance system data were used to determine incidence rates rather than using hospitalization registry data from selected hospitals, allowing for more stability. The results showed that exposure to PM2.5, PM10, NO2, and CO was associated with the incidence of ischemic stroke. This is similar to the results of a recent meta-analysis (Toubasi & Al-Sayegh, 2023).
Exposure to particulate matter pollutants of different particle sizes is associated with different levels of risk for ischemic stroke incidence and mortality. In the current study, PM2.5 was was associated with higher stroke incidence and mortality rate compared to PM10. Studies have shown that particulate pollutants with smaller particle sizes are more likely to enter the alveoli through respiration and cross the air-blood barrier into the circulatory system (Manojkumar, Srimuruganandam & Nagendra, 2019; Wang et al., 2021). This discussion on pollutant particle size is not applicable to all environments, and no such trend was found in the study by Li et al. (2023). This contradiction may be attributable to differences in pollutant concentrations in the study area. For cities with higher air pollution concentrations, public health policymakers should consider focusing on smaller particulate matter (like PM2.5 and PM1).
Unlike PM2.5 and PM10, this study did not find a significant effect of SO2 on the development of ischemic stroke in the overall population. However, further subgroup analyses showed that SO2 was significantly associated with ischemic stroke in those >75 years of age, whereas there was no significant association in those ≤75 years of age. This study also shows that age plays a modifying role in ischemic stroke-related mortality. This conclusion is supported by the available evidence that older individuals are more sensitive to air pollutants than younger populations (Luo et al., 2022). This may be related to lower immune responses and more prevalent comorbid underlying diseases in older individuals. Aging itself is one of the risk factors for poorer prognosis after stroke, and the rate of aging is a better indicator of the risk of stroke incidence than the age of the individual (Shao et al., 2020). In this study, season had a similar modifying effect on stroke incidence, and this may be attributed to poor diffusion conditions of pollutants during the cold season (Xu et al., 2022b). The physiological basis of the increase effect of air pollutants on stroke incidence during the cold season may be related to elevated blood pressure in the body and arterial thrombosis, which are both worsened by cold temperatures (Hong et al., 2003; Liu et al., 2021; Wang et al., 2016). The elderly population should have increased awareness of the risk of stroke incidence associated with air pollution, especially in winter when air pollutant concentrations are higher. However, not all epidemiologic studies are consistent in their findings. Studies from Israel and Poland support the conclusion that young people are more sensitive to air pollutants (Sade et al., 2015; Święczkowski et al., 2025). The study from Israel was conducted in a desert area, and the main pollutant was natural dust, whereas in the study from Poland the air pollution contained high levels of benzo(alpha)pyrene [B(a)P], which is quite different from the composition of the air pollutants in the current study. As mentioned above, both studies used hospital admission data rather than disease registry data, especially since only one hospital was covered in the study by Sade et al. (2015). This may lead to a large selection bias, with low rates of post-stroke morbidity treatment in the elderly population in relatively economically disadvantaged areas and a high rate of post-stroke morbidity and mortality in elderly patients further reducing admission rates.
The association between air pollution and ischemic stroke was stronger in females compared with males, and this is consistent with the results of certain previous study (Ban et al., 2021). However, in another study that did not rely on disease surveillance system registry data, ischemic stroke hospitalization due to air pollution was more strongly associated with male patients (Lv et al., 2023). This has again prompted researchers to emphasize the importance of obtaining data based on disease surveillance systems rather than focusing solely on registry data from selected hospitals. According to the World Stroke Organization (WSO), the proportion of stroke patients is higher in females (56% in 2019) than in males (Feigin et al., 2022), and females have a higher lifetime risk of stroke and worse stroke outcomes (Seshadri et al., 2006; Xu et al., 2022a). Hypertension is one of the most important risk factors for stroke. The dramatic increase in the prevalence of hypertension in postmenopausal females and the fact that stroke risk in females begins at a lower systolic blood pressure (SBP) threshold compared to males may increase the susceptibility to stroke in the female population (Ji et al., 2021; Mills et al., 2016). Additionally, specific risk factors in the female population such as pregnancy and exogenous estrogen intake also increase the risk of stroke (Swartz et al., 2017; Xu et al., 2015). To summarize, women, especially those of advanced age, are more susceptible to blood pressure, metabolic disorders, and abnormal hormone levels, ultimately increasing the risk of stroke associated with air pollution.
Most of the previous research on this topic examined the effect of air pollution on either stroke incidence or mortality in specific populations, and studies have rarely included both outcomes. By using the DLNM, this study more intuitively explores these relationships. This study found an earlier increase in the risk of air pollution-related stroke mortality prior to the increased risk of air pollution-related stroke incidence. The risk of ischemic stroke-related mortality due to PM2.5, PM10, and CO increases at lag0, excluding NO2. This again suggests that health policy makers should address the loss of life due to air pollution-related stroke. In the single-day lagged structures, a strong association was found between NO2 and the risk of stroke incidence, but only a tiny association between NO2 and the risk of stroke mortality was observed. Tian et al. (2022) retrieved 318,752 subjects from the UK Biobank to study the effects of particulate matter pollutants (PMx) and nitrogen oxides (NOx) on the various stages of stroke progression and showed that, for every five µg/m3 increment in PM2.5 and NO2, there was a 30% and 3% increase, respectively, in the risk of the population transitioning from a healthy state to mortality, and that NO2 associated with stroke deaths with minimal intensity. In another study, death rates after intravenous thrombolysis (IVT) for stroke were highly associated with short-term exposure to particulate matter (PM), but not to NO2 (Cappellari et al., 2018). The health effects of short-term exposure to NO2 have been systematically reviewed by Hesterberg et al. (2009) who concluded that the concentration at which NO2 produces extrapulmonary effects is generally higher than 1–2 ppm (about 2,000–4,000 µg/m3 at standard state). In Zhu et al. (2012) the nitrogen dioxide concentration was set to extremely high levels, far exceeding real-world concentrations. The maximum concentration in the current study was only 49.8 µg/m3, which is much lower than the 2,000 µg/m3 that may produce extrapulmonary hazards. Additionally, in the current study, NO2 was no longer associated with stroke incidence in a two-pollutant model adjusted for PM2.5 and PM10 separately. It is reasonable to doubt whether there is a real association of NO2 with stroke incidence or whether this association is due to collinearity. Additional evidence from clinical studies is still needed to address this issue.
As discussed above, collinearity may confound the effect of NO2, representing one of the limitations of this study. Li et al. (2022) investigated the health effects of air pollution mixtures on the overall death rate in the elderly individuals using Bayesian kernel machine regression (BKMR). This model allows for flexible capture of joint effects of mixture components, thereby capturing potential interactions and nonlinear effects. Future studies may consider using alternative machine learning models to distinguish between the impact of individual pollutants and the overall effect of mixtures on stroke incidence or mortality, thus providing more robust evidence for health decision-making.
Conclusions
In this time series study involving 209,949 individuals registered in the disease surveillance systems dataset, short-term exposure to air pollution (PM2.5, PM10, SO2, NO2, and CO) was significantly associated with the increased risk of ischemic stroke incidence and mortality. Elderly populations are more sensitive to exposure to air pollution and have a higher risk of ischemic stroke incidence and mortality compared to the non-elderly. In addition to age factors, this study shows that air pollutants have a different impact on the incidence of stroke in different genders, with the association between air pollution and ischemic stroke being stronger in women than in men. It is particularly important to address the impact of air pollution on the elderly and women in clinical practice.
Supplemental Information
RRs (%) and 95% CIs for the effect of air pollution on ischemic stroke incidence and mortality by subgroup in stratified analysis
Spearman’s correlation coefficients between air pollutants and temperature
Relative risk of ischemic stroke death associated with air pollution exposure stratified by sex, age, and season of death time in a single lag day structure
Red color indicates the association was significant. RRs and 95 % CIs were calculated for each IQR increment
Relative risk of ischemic stroke death associated with air pollution exposure stratified by sex, age, and season of death time in a cumulative day structure
Red color indicates the association was significant. RRs and 95% CIs were calculated for each IQR increment.