
Factors affecting molar root and periodontal hard tissue changes after orthodontic anterior molar closure of missing tooth spaces retrospective explored based on cone-beam computed tomography three-dimensional reconstruction
- Published
- Accepted
- Received
- Academic Editor
- Jincheng Wang
- Subject Areas
- Dentistry, Radiology and Medical Imaging
- Keywords
- Molar anterior displacement, Alveolar bone loss, Cone beam computed tomography (CBCT), Root volume, Root resorption
- Copyright
- © 2025 Huang et al.
- Licence
- This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits using, remixing, and building upon the work non-commercially, as long as it is properly attributed. For attribution, the original author(s), title, publication source (PeerJ) and either DOI or URL of the article must be cited.
- Cite this article
- 2025. Factors affecting molar root and periodontal hard tissue changes after orthodontic anterior molar closure of missing tooth spaces retrospective explored based on cone-beam computed tomography three-dimensional reconstruction. PeerJ 13:e18875 https://doi.org/10.7717/peerj.18875
Abstract
Objective
To correlate the molar teeth and their periodontal conditions after orthodontic anterior removal of the molars to close the gap of missing teeth and to provide risk factor analysis and prognostic assessment for the treatment of such cases.
Methods
Twenty-six orthodontic patients (five males and 21 females) with a total of 42 teeth were selected to undergo full-mouth orthodontic treatment due to the absence of the first/second molar and the molar bone volume was recorded by cone-beam computed tomography (CBCT) scanning before (T0) and after (T1) the treatment, and the root volume and the bone volume of the molar teeth were calculated by three-dimensional reconstruction of the CBCT. Afterwards, the correlation analysis was performed between the molar root volume change and bone volume condition and age, gender, density, width, height of the alveolar bone in the edentulous area, edentulous gap and root condition.
Results
The amount of alveolar bone loss and root resorption in the anteriorly displaced molars after treatment was less than 20%. There was a statistically significant correlation between age and pre-treatment periodontal condition, distal mesial and buccal bone loss; there was a statistically significant correlation between alveolar bone width in the edentulous area and pre-treatment periodontal condition and buccal bone loss; there was a statistically significant correlation between edentulous gap and post-treatment periodontal changes and buccal bone loss; there was a statistically significant correlation between gender and lingual bone loss; and there was a statistically significant correlation between root resorption and pre-treatment There was a statistically significant correlation between the width of the alveolar bone in the edentulous area; there was no statistically significant correlation between the density and height of the alveolar bone in the edentulous area and the periodontal condition.
Conclusion
Closure of the missing gap by orthodontic proximal-medial movement of the molar is a feasible method, but we need to pay close attention to the width of the alveolar bone and the missing space in the edentulous area.
Introduction
The surface of molar teeth has many fossae and grooves, which is easy to caries, and if not treated in time after caries, it is difficult to repair and eventually lead to extraction. Molar teeth play an important role in mastication, and the premature loss of molar teeth will cause a reduction in the efficiency of mastication, concentration of stress on the remaining molar teeth, leading to temporomandibular joint dysfunction, and then the emergence of asymmetry of the jaw shape and other aspects of the harm (Katta & Kakkunath Mani, 2020; Sakai & Yamashita, 2021). Currently, the main methods for repairing missing teeth gap are removable denture restoration, bridge restoration, implant restoration, orthodontic movement to close the gap and autogenous tooth replantation. And the implant and orthodontic restorations are more and more widely used. However, the indications for implant restorations are strict, and most patients with missing molar teeth have insufficient gaps due to the long period of absence (Cardoso, Mecenas & Normando, 2022). Orthodontic restoration utilizes the movement of natural teeth to close the gap, which has relatively wider indications and retains the sensory function of natural teeth, better biocompatibility, infection resistance and other advantages (Cárcamo-España et al., 2022).
The current problem is that in cases where the molar teeth are moved forward to close the gap, the alveolar bone resorption in the edentulous area is generally severe, and whether the long-distance movement will result in the resorption of the tooth root, the loss of alveolar bone volume, resulting in the deterioration of the periodontal condition of the molar teeth. Some studies have found that root resorption is related to the distance of tooth movement, but the safe distances in the horizontal and vertical directions are still unclear (Aman et al., 2023; Li et al., 2022). A previous study found that there is a risk of bone dehiscence bone windowing when the root moves into the buccolingually oriented alveolar ridge that is narrower in width than the root (Wu et al., 2023). However, some studies have also found that an increase in alveolar bone volume occurs after movement of this type of tooth (Cardoso, Mecenas & Normando, 2022). There are very few studies on the correlation between root and periodontal changes in molar teeth after movement to close the gap and the risks and risk factors for treatment are unclear.
Therefore, in this experiment, cone-beam computed tomography (CBCT) was used for volume and length measurements, and the pre-treatment root and alveolar bone conditions and the post-treatment root and alveolar bone conditions were measured, respectively, and the periodontal changes before and after treatment were analyzed using the alveolar bone conditions. The patients’ alveolar bone base condition and periodontal changes in the edentulous area were correlated and analyzed, and the relationship between periodontal changes, the amount of alveolar bone loss and root volume changes in the four sites of the molar proximal and distal buccal and lingual sides, and the relationship between the age, gender, the density, width, and height of the alveolar bone in the edentulous area, the edentulous gap, and the root condition were analyzed, so as to provide references for the clinical prognostic assessment.
Materials and Methods
Study population
The study was conducted in accordance with the Declaration of Helsinki (revised in 2013) and approved by the Ethics Committee of the Third Affiliated Hospital of Sun Yat-sen University (No. II2024-197-01), and patients were screened for enrollment by an orthodontist based on the following criteria. Included in the study were 26 orthodontic patients (five males and 21 females) with 42 teeth who came to the Third Affiliated Hospital of Sun Yat-sen University for orthodontic treatment from May 1, 2020 to April 30, 2022 and who needed to have their molar teeth moved forward to close the missing tooth gap. All enrolled patients have signed informed consent forms, agreeing that case data can be used for teaching and clinical research. Inclusion criteria: (1) no periodontal disease; (2) no systemic disease; (3) no history of smoking; (4) proximal and distal mesial gaps in the edentulous area were ≥8 mm (Zhuo, Jiang & Di, 2020); (5) age over 18 years; (6) no history of oral treatment for the moved molars. Exclusion criteria: (1) periodontal probing depth of >4 mm; (2) alveolar bone resorption greater than 1/3 of the root; (3) not having good oral hygiene habits; (4) elevated or depressed molar treatment during treatment; (5) severe bone windowing and cracking of bone during treatment; (6) failure to reduce the gap for more than 3 months or failure to completely close the gap; and (7) root resorption greater than 20% of the original volume. All subjects were fully informed about the oral hygiene maintenance program. Oral hygiene education and health checkups were conducted at each follow-up visit. CBCT was taken before and after treatment.
Treatment procedure
Each patient underwent anterior molar closure of the gap using the same treatment protocol and no elevating and depressing molar manipulation during treatment, and the same CBCT (large field of view) (NewTom Vgi, Cone Beam CT, Safelite, Italy, voltage 110 kV, current 1–20 mA, layer thickness spacing 0.3 mm) was used to collect imaging data from the beginning of the treatment (T0) and the end of the treatment for each patient (T1) imaging data. Patients were rechecked every 4 weeks, and tooth movement and periodontal condition were examined at each visit until the end of orthodontic treatment.
Measurement of the amount of alveolar bone height loss in the edentulous area, edentulous gaps, density, and width
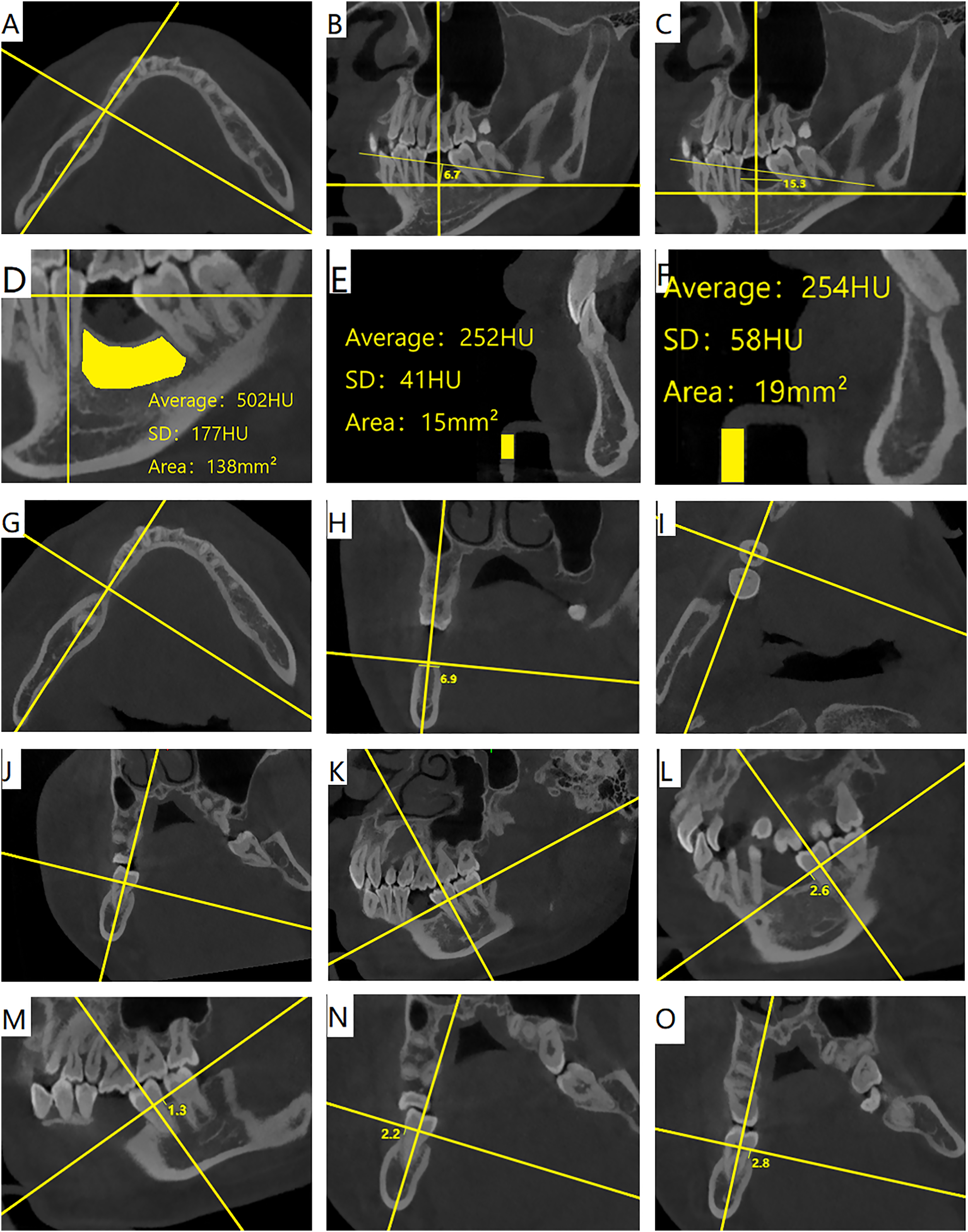
Using the software NNT Viewer software (Version 11.5), adjusted to the horizontal plane view, made a proximal and distal mesial cross-section of the top of the alveolar ridge equally divided in the edentulous area (Fig. 1A), made a line within the cross-section of the adjacent enamel-osteoplastic boundary at the gap, and measured the maximum vertical distance from the top of the alveolar ridge to the line (Fig. 1B) as the amount of the missing alveolar bone height of the edentulous area; and measured the amount of the missing alveolar bone height of the edentulous area before the treatment. The line between the proximal and distal midpoints of the adjacent teeth and the intersection point of the alveolar bone was measured as the length of the gap (Fig. 1C); the alveolar bone density values at the gap were measured (Fig. 1D), and the density values of the CBCT reference were measured before and after the treatment (Figs. 1E and 1F), respectively, to correct for the before- and after-treatment CBCT densities; buccolingual cross-sections perpendicular to the alveolar ridge were made at the narrowest point of the alveolar crest of the missing tooth area (Fig. 1G), and coronal profiles of the alveolar crest were obtained (Fig. 1H), and the length of the bottom edge of the top arc of the alveolar ridge was measured (Fig. 1H) as the width of the alveolar bone.
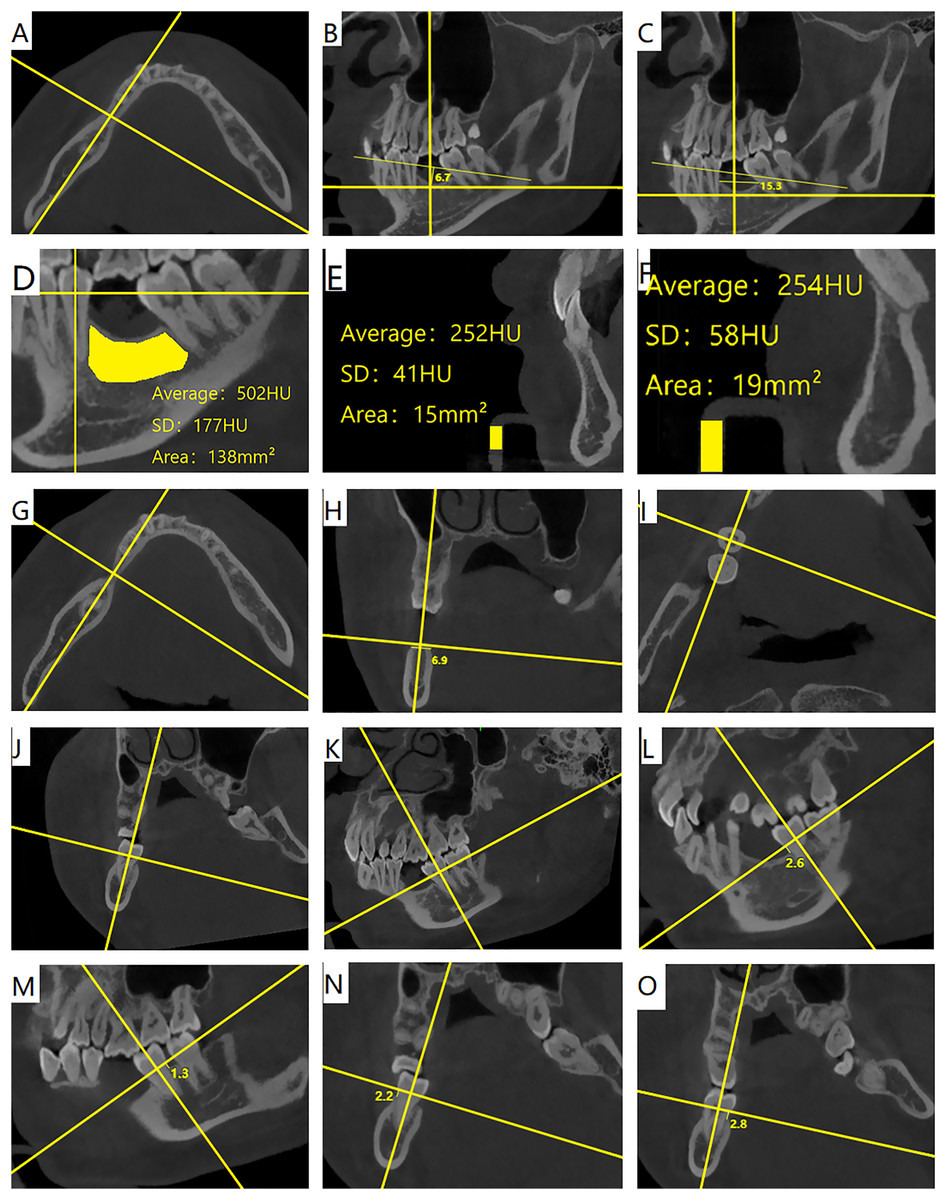
Figure 1: (A) Horizontal plane view, making a proximo-distal mesial section equally divided by the top of the alveolar ridge in the edentulous area. (B) Making a line connecting the adjacent enamel-osteoskeletal boundaries in the edentulous area, and measuring the maximum perpendicular distance from the top of the alveolar ridge to the line/mm. (C) Length of the edentulous area before treatment/mm. (D) Measuring the density of alveolar bone in the edentulous area. (E) Measuring the density of the pre-treatment CBCT reference. (F) Measuring the density of the post-treatment CBCT reference. (G) Horizontal plane view, the Buccolingual section perpendicular to the alveolar ridge at the narrowest point of the alveolar ridge in the edentulous area. (H) Coronal section of the alveolar ridge, measurement of the width of the top of the alveolar ridge/mm. (I) Horizontal plane view. (J and K) Planar adjustment to the segmented enamel-osteoskeletal boundary. (L–O) Distance from the top of the top of the alveolar ridge at the highest point of the alveolar ridge to the enamel-osteoskeletal boundary at the four sites of the proximal-medium (L), distal-medium (M), buccolingual (N), and lingual (O)/mm.
{kind=link}
Measurement of bone height loss in anteriorly displaced molars
Using the software NNT Viewer software (Version 11.5), the planes were adjusted to divide the enamel bone boundary (Figs. 1I–1K), The distance from the highest point of the alveolar ridge apex to the enamel bone border, as attachment loss (AL), and the AL was measured for the four pre-treatment proximal-medial (Fig. 1L), distal-medial (Fig. 1M), buccal (Fig. 1N), and lingual (Fig. 1O) sites. AL was measured as S0 before treatment, S1 after treatment, and the amount of molar bone height loss S = S0–S1.
Volumetric measurements
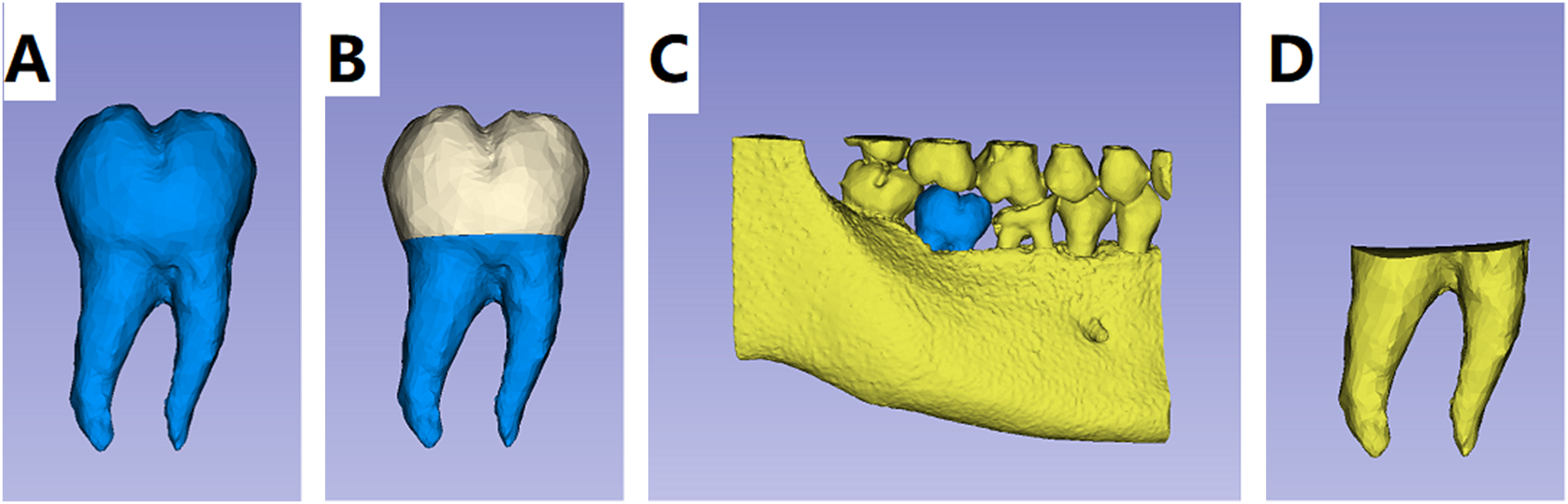
CBCT was analyzed using the open source software 3D Slicer (version 5.7.0) (Fedorov et al., 2012; Ramos et al., 2020), and reference density values were measured to correct for pre- and post-treatment CBCT density. The molar roots and alveolar bone were segmented using a threshold. (1) The pre-treatment volume of the tooth V0 and the post-treatment volume V1 were measured (Fig. 2A). The crowns and roots were segmented along the enamel dental bone boundary, and the pre-treatment root volume Vr0 and the post-treatment root volume Vr1 were measured and the root resorption volume (EARR) was calculated (Mashyakhy et al., 2022) (Fig. 2B). The EARR was calculated as (Vr1 − Vr0)/Vr0 × 100%. (2) The roots were assembled with the alveolar bone and separated from the pre-treatment sub-alveolar bone roots using automatic and manual segmentation to measure the volume Vp0 and the post-treatment sub-alveolar bone roots and measure the volume Vp1 (Figs. 2C, 2D), and the pre-treatment periodontal condition ratio was calculated as PC0 = Vp0/V0 × 100%. Post-treatment periodontal condition ratio PC1 = Vp1/V1 × 100%. Calculate the change in periodontal ratio before and after treatment defined as periodontal change condition PC (Periodontal Condition) = PC1–PC0.
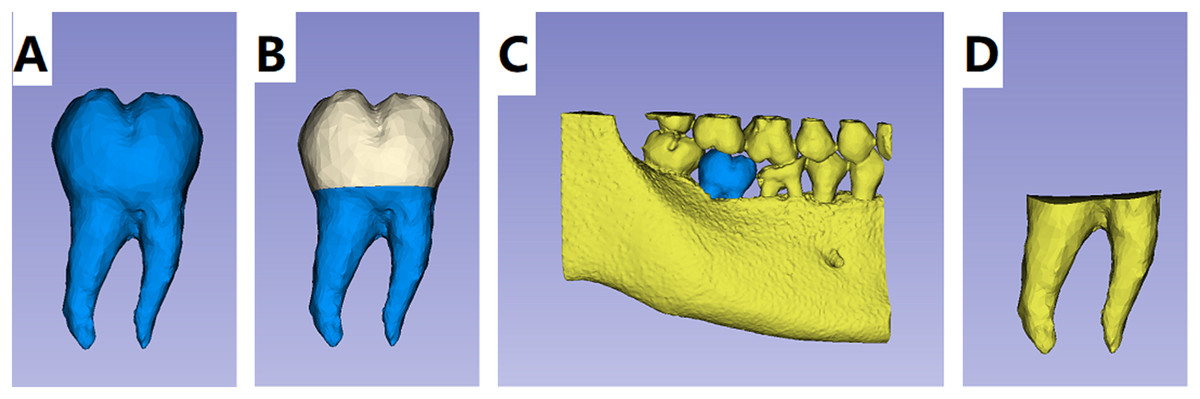
Figure 2: (A) Segmentation of molar root. (B) Segmentation of crown and root along the enamel-osteum boundary. (C) Root and alveolar bone assembly. (D) Separation of the root from the alveolar bone.
{kind=link}
Data collection
CBCT images were all taken by the same operator using the same equipment before and after patient treatment, and all measurements were processed and averaged three times by the same researcher. In the pre-experiment, the same researcher used 3D Slicer (Version 5.7.0) for volumetric measurements, NNT Viewer (Version 11.5) for length measurements, and SPSSAU (Version 24.0) for ICC analysis and the results were as follows: Table 1, shows that the volumetric measurements were highly reliable. Table 2, shows that the length measurements were highly reliable.
| One-way absolute agreement | ICC intragroup correlation factors | 95% CI |
|---|---|---|
| Single measures ICC (1) | 1.000 | [1.000–1.000] |
| Average mesures ICC (K) | 1.000 | [1.000–1.000] |
Note:
1: a single measure, K: an average measure
| One-way absolute agreement | ICC intragroup correlation factors | 95% CI |
|---|---|---|
| Single measures ICC (1) | 0.996 | [0.989–0.999] |
| Average mesures ICC (K) | 0.999 | [0.996–1.000] |
Note:
1: a single measure, K: an average measure
Statistical analysis
SPSS 25.0 software was used to statistically analyze the measured data. Because no study has been conducted so far to compare the loss of root volume under the anteriorly displaced alveolar bone of the molars before and after treatment, sample size estimation was performed by a pre-experiment before the study began. The inclusion criteria of the pre-experiment were the same as in the present study, and seven teeth were selected for data analysis; the mean value of post-treatment EARR was −3.21% with a standard deviation of 4.77%, and the mean value of post-treatment periodontal changes was −10.26% with a standard deviation of 5.49%, and according to the computational analysis, when the two-sided α = 0.05 and the test efficacy of 90%, the minimum sample size was 35, and the data normality was determined by using the S-W test and the Q-Q plot to test the normality of the data, paired-sample t-test for the data before and after treatment, Mann-Whitney-U nonparametric test for the influence of gender and root condition on post-treatment tooth grinding, and Spearman’s correlation analysis for the correlation between patient’s age, the proportion of root volume under the alveolar bone, the height and width of the alveolar bone in the edentulous area, the missing teeth gap, and the density of the teeth, and the post-treatment tooth grinding, were used. A two-by-two correlation analysis was performed to analyze the proportion of sub-alveolar bone root volume and proportional change, the proportion of root resorption, and the amount of bone loss at four sites in the proximal, distal, mesial, buccolingual, and lingual sides of the anteriorly displaced molar teeth.
The test level was two-sided α = 0.05. For correlation coefficient r analysis, when | r | ≥ 0.8, it was regarded as highly correlated, when 0.8 > | r | ≥ 0.5, it was regarded as moderately correlated, when 0.5 > | r | ≥ 0.3, it was regarded as lowly correlated, and when | r | was less than 0.3, it was regarded as weakly correlated or not correlated (Gupta et al., 2023).
Results
All 42 teeth in the study had a post-treatment EARR of less than 20% and met the inclusion criteria, with 8 (19.05%) having an EARR ≤ 0, 28 (66.67%) having an EARR > 0 and <10%, and 6 (14.29%) having an EARR ≥ 10% and <20% (Table 3).
| EARR degree | Quantity/pc | Percentage/% |
|---|---|---|
| ≤0% | 8 | 19.05 |
| >0% and <10% | 28 | 66.67 |
| ≥10% and ≤20% | 6 | 14.29 |
| >20% | 0 | 0 |
The mean value of bone height loss at the four sites (proximal-medial, distal-medial, buccal, and lingual) after the molar movement into the edentulous space after treatment was less than 1 mm (Table 4). The total number of 168 sites was analyzed with respect to the bone height of each site (Table 5). A total of 25% of the sites had an increase in bone height, 13.69% had no change in bone height, 72.61% had a loss of bone height of less than 1 mm, 92.85% had a loss of bone height of less than 2 mm, 97.61% had a loss of bone height of less than 3 mm, and the highest site was 5.30% with a loss of bone height of less than 1 mm. The highest locus was 5.30 mm. According to the observation of post-treatment CBCT, there was a slight bone dehiscence on the buccolingual side of some of the teeth, but no bone windowing was found.
| Measurement site | The amount of bone height lost | |
|---|---|---|
| Average | Median | |
| Proximal | 0.32 | 0.15 |
| Distal | 0.39 | 0.05 |
| Buccal | 0.65 | 0.60 |
| Lingual | 0.80 | 0.60 |
| The amount of bone height lost | Number of included bits/pc | % |
|---|---|---|
| <0 mm | 42 | 25.00 |
| =0 mm | 23 | 13.69 |
| 0~mm | 57 | 33.92 |
| 1~mm | 34 | 20.24 |
| 2~mm | 8 | 4.76 |
| 3~mm | 1 | 0.60 |
| 4~mm | 2 | 1.20 |
| 5~6 mm | 1 | 0.60 |
| Total | 168 | 100 |
The ratio of root volume to total tooth volume under the alveolar bone was defined as the periodontal condition ratio, and the change in the periodontal ratio before and after treatment was calculated and defined as the periodontal change condition PC (periodontal condition). An increase in the PC predicted better periodontal condition and a decrease in the PC predicted poorer periodontal condition, and in this study the periodontal condition was elevated and unchanged in 11.90% of the cases, and periodontal condition was decreased by 10% or less in 52.38%, and decreased by more than 10%. A total of 52.38%, and reduction of more than 20% was zero (Table 6).
| Groups | Quantity | % | |
|---|---|---|---|
| Elevated | 4 | 9.52 | |
| Unchanged | 1 | 2.38 | |
| Decrease >0% and ≤10% | 22 | 52.38 | |
| Decrease >10% and ≤20% | 15 | 35.71 | |
| Decrease >20% | 0 | 0 | |
Note:
PC indicates the periodontal change as the change in periodontal ratio before and after treatment. Periodontal ratio is the ratio of root volume to total tooth volume under the alveolar bone.
A pair-wise correlation test of the measured data before and after treatment showed that r > 0.4 and P < 0.01, indicating a significant correlation between the paired samples, and a pair-wise t-test showed that (Table 7), there was a statistically significant difference in the amount of root resorption, periodontal changes, and the amount of distal-medial, buccal, and lingual bone loss between before and after treatment (P < 0.05). However, the amount of proximal-medial bone loss before and after treatment was not statistically different (P > 0.05).
| Vr1-Vr0 | Vp1-Vp0 | PC1-PC0 | The amount of medial loss | The amount of distal loss | The amount of buccal loss | The amount of lingual loss | |
|---|---|---|---|---|---|---|---|
| P | 0.00 | 0.00 | 0.00 | 0.07 | 0.02 | 0.00 | 0.00 |
Notes:
Vr0: the pre-treatment root volume; Vr1: the post-treatment root volume. Vp0: the pre-treatment subalveolar roots volume; Vp1: the post-treatment subalveolar roots volume. PC0: the pre-treatment periodontal ratio; PC1: the post-treatment periodontal ratio. At the 0.05 level (two-tailed), the correlation is significant.
Significant at the 0.01 level (two-tailed).
Correlation analysis of the basal condition of the edentulous area before treatment and the periodontal condition after treatment and the difference in the amount of bone loss before and after treatment at the four sites (Table 8) showed that there was no statistically significant correlation between the EARR and age, alveolar bone width in the edentulous area before treatment, the loss of height, density, and the gap of edentulousness (P > 0.05). There was no statistically significant correlation between the amount of alveolar bone height loss and density in the edentulous area and the ratio of periodontal conditions before and after treatment, periodontal changes, and the amount of bone loss in the distal-medial and buccolingual three loci (P > 0.05). There was no statistically significant correlation between age at treatment and post-treatment periodontal condition ratio, periodontal changes, and amount of lingual loss (P > 0.05), and there was a statistically significant correlation with the amount of distal-medial and buccolingual loss (P < 0.05), corresponding to correlation coefficients of 0.31 and 0.36, respectively, whereas there was a statistically significant correlation (P < 0.01), corresponding to a correlation coefficient of −0.48. There was no statistically significant correlation between the width of the alveolar bone in the edentulous area and the post-treatment periodontal condition ratio, periodontal changes, and the amount of distal-medial and lingual loss (P > 0.05), while there was a statistically significant correlation with the pre-treatment periodontal condition ratio (P < 0.05), corresponding to a correlation coefficient of 0.32, and a statistically significant correlation with the amount of buccal bone loss (P < 0.01), corresponding to a correlation coefficient of −0.44. There was no statistically significant correlation between the missing tooth gap and the ratio of periodontal conditions before and after treatment and the amount of distal-medial and lingual loss (P > 0.05), there was a statistically significant correlation with the amount of loss on the buccal side (P < 0.05), corresponding to a correlation coefficient of 0.31, and there was a statistically significant correlation with the periodontal changes (P < 0.01), corresponding to a correlation coefficient of −0.45.
| Correlation coefficient | EARR | PC0 | PC1 | PC | The amount of distal | The amount of buccal loss | The amount of lingual loss |
|---|---|---|---|---|---|---|---|
| Age | 0.16 | −0.48** | −0.30 | −0.09 | 0.31* | 0.36* | 0.10 |
| Alveolar bone width in edentulous area | 0.17 | 0.32* | 0.22 | 0.03 | −0.14 | −0.44** | −0.11 |
| Loss of alveolar bone height in the edentulous area | −0.25 | 0.01 | 0.02 | 0.05 | −0.13 | −0.08 | −0.13 |
| Gap between missing teeth | −0.14 | 0.22 | −0.17 | −0.45** | 0.29 | 0.31* | 0.16 |
| Alveolar bone density in the edentulous area | 0.13 | −0.05 | 0.02 | 0.06 | −0.07 | 0.05 | −0.08 |
Note:
PC indicates the periodontal change profile, which is the change in periodontal ratio before and after treatment. *Correlations are significant at the 0.05 level (two-tailed).**At the 0.01 level (two-tailed), the correlation is significant.
Non-parametric tests and correlation analysis (Table 9) for gender, root residue, yielded a statistically significant difference between different genders and the amount of bone loss in the distal mesocolon (P < 0.05), with greater loss in females than in males, corresponding to a correlation coefficient of 0.34. There was a statistically significant difference between different root residues and pre-treatment alveolar bone width (P < 0.01), and the pre-treatment width of alveolar bone with roots was greater than that of rootless alveolar bone, corresponding to a correlation coefficient of 0.43.
| Gender and amount of distal mesial bone loss | Root condition and pre-treatment alveolar bone width | |
|---|---|---|
| Mann-Whitney-U test Z-value | −2.20 | −2.76 |
| P | 0.03 | <0.01 |
| Spearman correlation analysis r-value | 0.34* | 0.43** |
Note:
*At the 0.05 level (two-tailed), the correlation is significant. **Significant at the 0.01 level (two-tailed).
Discussion
Some studies have found that there is a high risk of root resorption in cases of long-distance orthodontic tooth movement. Li et al. (2022), and according to Liu et al. (2021) who graded the degree of EARR (Mashyakhy et al., 2022). In this study, 42 teeth were treated with EARR less than 20% and no severe root resorption was found, of which 19.05% had no root resorption, 66.67% had mild root resorption, and 14.29% had moderate root resorption, Li et al. (2020) also found that 18.16% of teeth had no root resorption in fixed orthodontic treatment, 61.79% had mild root resorption, 19.24% teeth showed moderate root resorption and 0.81% teeth showed severe root resorption. In the correlation analysis, no statistically significant correlation was found between the condition of the missing tooth area and root resorption in the patients. It suggests that although there is a risk of root resorption in long anteriorly displaced molar closure gaps, the degree of resorption is at a relatively safe level and the prognosis is good.
Loss of alveolar bone height is one of the causes of bone dehiscence, and in this study buccolingual bone loss was generally higher than proximal and distal mesial, and paired t-test analysis yielded no statistically significant changes in proximal mesial bone height before and after treatment. By post-treatment CBCT, slight bone dehiscence was observed on the buccolingual side of some teeth, but no bone windowing was found. This suggests that loss of bone height is at risk and more common on the buccolingual side, which is prone to bone dehiscence. Nonetheless, 25% of the loci showed bone gain after treatment, 13.69% showed no change in bone height, and 97.61% of the loci showed a loss of bone height of less than 3 mm. Correlation analysis suggested that the loss of bone height was related to gender age, width of alveolar bone in the edentulous area and distance of movement. Lund, Gröndahl & Gröndahl (2012) found that the mean value of alveolar bone height loss in the lower anterior teeth in adolescents treated with orthodontics was 0.3 mm more in girls as compared to boys (Wang et al., 2023). Schubert et al. (2020) found that with increasing age, the activity of osteoclasts and osteoblasts in the alveolar bone decreases, the bone resorption and bone. The decrease in bone resorption and bone formation, and the decrease in bone remodeling capacity make it more likely to experience a high degree of alveolar bone loss. Grimoud, Gibbon & Ribot (2017) observed that the prevalence of bone dehiscence has a slight increase in people over 30 years of age in a study of 1,175 teeth (Nalbantoğlu & Yanık, 2023). A related analysis also indicated a negative correlation between age and pre-treatment periodontal condition. Pereira et al. (2024) showed that there is a risk of bone dehiscence when the root moves into the alveolar ridge which is narrower than the buccolingual width of the root (Wu et al., 2023). There was a statistically significant correlation between alveolar bone width in the edentulous area prior to treatment and root survival, which is more favorable for the preservation of alveolar bone width. Therefore, pre-treatment assessment of gender, root survival, age, alveolar bone width in the edentulous area, and edentulous gap is informative in predicting the amount of alveolar bone loss.
In this study, the periodontal condition of the tooth was described by analyzing the ratio of the volume of the root under the alveolar bone to the total tooth volume, and the periodontal condition before and after treatment was compared to derive the periodontal change PC, with an increase in PC predicting a better periodontal condition and a decrease in PC predicting a worse periodontal condition. In this study, the periodontal conditions of 42 teeth were not reduced by more than 20%, and the periodontal conditions were elevated by 9.52% and the PC was unchanged by 2.38%, and the periodontal conditions were reduced by less than 10% by 52.38%, suggesting that closing the gap between the missing teeth through orthodontic proximal and intermediate removal of molars will not cause serious periodontal damage, and even an improvement in the periodontal conditions will occur. Aman et al. (2023) also found that no serious periodontal destruction and an increase in bone height at individual sites were found after closing the edentulous space with orthodontic proximal and intermediate removable molar. With correct orthodontic forces and in the absence of periodontitis, molar bone remodeling occurs during orthodontic movement and new bone attachments are formed. Lindskog-Stokland et al. (2013) found that regeneration of alveolar bone is possible when teeth are moved to the alveolar bone in the edentulous region through case studies (Liu et al., 2021).
In this study, alveolar bone density and height in the edentulous area did not suggest treatment risk, but periodontal changes and the amount of molar bone loss correlated with gender, root condition, age, alveolar bone width in the edentulous area, and the edentulous gap, suggesting that the assessment of the patient’s molar teeth prior to treatment has prognostic significance. For some patients who are unable to undergo implant restoration due to low alveolar bone, orthodontic restoration of the missing gap can be attempted, but the prognosis needs to be evaluated according to the condition of the missing teeth area before treatment, and the possible risks should be paid attention to.
This study used CBCT for 3D reconstruction to calculate the volume of tooth roots and alveolar bone. Most previous studies used panoramic or apical radiographs to assess root length and alveolar bone height, but two-dimensional imaging leads to compression and distortion of the images (Aman et al., 2023). Root resorption and alveolar bone loss exhibit complex three-dimensional changes, extending beyond linear measurements in 2D imaging, and it has been found that root length may not change significantly when root volume changes (Kalina, Grzebyta & Zadurska, 2022). The CBCT three-dimensional imaging modality overcomes these drawbacks. It has also been demonstrated that in vivo CBCT and post-extraction in vitro micro-computed tomography (Micro-CT) are well comparable in terms of accuracy of volume measurements (Intarasuksanti et al., 2023; Su et al., 2023).
Since in this type of cases, the neighboring teeth tend to be tilted to the side of the gap, in this study the gap was measured as the line between the proximal and distal intersections of the neighboring teeth on both sides and the alveolar bone before treatment. In the correlation analysis, the gap was negatively correlated with periodontal changes and positively correlated with the amount of bone loss on the buccal side. In this study, the average gap was 12.44 mm, and the maximum gap was 16.90 mm, without severe periodontal destruction and severe bone cracking and with a good prognosis. Bone loss on the buccal side is prone to bone dehiscence (Pereira et al., 2024), and the evaluation of the gap before treatment is of reference significance to the prognosis, and patients with a large gap need to pay more attention to periodontal changes and root-bone relationship during treatment to avoid bone dehiscence and bone cracking.
Since this study is a retrospective study, it is not possible to collect oral hygiene and periodontal indices of patients during treatment. A prospective study can be conducted to include patients’ oral hygiene and periodontal indices, etc., in the analysis of factors influencing alveolar bone changes.
Conclusion
Closure of the missing gap by orthodontic proximal-medial movement of the molar is a feasible method, but we need to pay close attention to the width of the alveolar bone and the missing space in the edentulous area.