
Work-related musculoskeletal disorder and health risk behaviors in market-vendors: a mixed-methods study
- Published
- Accepted
- Received
- Academic Editor
- Priyanka Banerjee
- Subject Areas
- Kinesiology, Orthopedics, Public Health, Mental Health, Rehabilitation
- Keywords
- Work-related musculoskeletal disorders, Health risk behaviors, Market-vendors, Muscle pain, Alcohol consumption, Drug misuse, Muscle flexibility, Physical inactivity
- Copyright
- © 2024 Cetthakrikul and Perngparn
- Licence
- This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits using, remixing, and building upon the work non-commercially, as long as it is properly attributed. For attribution, the original author(s), title, publication source (PeerJ) and either DOI or URL of the article must be cited.
- Cite this article
- 2024. Work-related musculoskeletal disorder and health risk behaviors in market-vendors: a mixed-methods study. PeerJ 12:e18079 https://doi.org/10.7717/peerj.18079
Abstract
Background
Work-related musculoskeletal disorders (WRMDs) are frequently observed among market vendors, and engaging in health risk behaviors can exacerbate these issues, leading to various health problems. Common health risk behaviors among market vendors include alcohol consumption and insufficient physical activity. However, there is currently a lack of research examining the prevalence of WRMDs and health risk behaviors among market vendors in Bangkok. Furthermore, the emerging trend of drug misuse within this group remains poorly understood. This study aims to explore the prevalence of muscle pain and flexibility issues and assess health risk behaviors, including alcohol consumption, inadequate exercise, and drug misuse, among market vendors.
Methods
A mixed-method study was undertaken among 213 market vendors in Bangkok. Data collection utilized direct observation techniques, questionnaires, and muscle flexibility tests. Qualitative data were elucidated and showcased through textual descriptions and quotations. Quantitative data were analyzed using descriptive statistics to present numerical and percentage values.
Results
Qualitative findings revealed that market vendors often engage in static muscular work and maintain awkward postures due to their job characteristics and workstation setups. Quantitatively, the right arm was the most common pain region (34.7%), followed by the left leg (31.0%), right leg (30.0%), and left arm (28.6%). Additionally, 64.3% of participants showed poor muscle flexibility. The study also found that 35% of market vendors resorted to alcohol and 11.7% to drug misuse to cope with fatigue and prevent adverse symptoms. Moreover, 68.5% of participants reported no regular exercise due to lack of time.
Conclusion
The study highlights the prevalence of musculoskeletal issues among market vendors, largely attributed to static muscular work and awkward postures dictated by their job roles and workstation arrangements. The right arm emerged as the most commonly affected area, followed by the left leg, right leg, and left arm, with significant rates of reported pain. The research also points to a notable lack of muscle flexibility in a majority of vendors and a concerning tendency towards alcohol and drug misuse as coping mechanisms for fatigue and symptom management. Furthermore, a significant portion of the vendors do not participate in regular exercise, primarily due to time constraints. These findings can be used to implement health prevention programs within the market vendor group.
Introduction
Work related musculoskeletal disorders (WRMDs) often occur in market vendors because of job characteristics such as prolonged sitting and standing, repetitive arm movement and lifting a heavy load. The common symptoms of WRMDs include muscle pain, muscle discomfort, muscle fatigue, muscle weakness and loss of muscle flexibility (European Agency for Safety and Health at Work, 2008). Previous research identified three main factors associated with WRMDs in workers: external factors such as repetitive tasks, poor posture, and heavy lifting; personal factors including age, smoking, alcohol consumption, obesity, and pre-existing medical conditions; and psychosocial factors such as lack of job control, high job pressure, and poor communication (Canadian Centre for Occupational Health and Safety, 2014; European Agency for Safety and Health at Work, 2008; Mahendran & Tiwari, 2023). The consequences of WRMDs can impact physical health, mental health, and work ability (Briggs et al., 2018; Zhang et al., 2015). In Thailand, the Department of Labor Protection and Welfare reported that 84.54% of workers had to cease working, quit their jobs, or take sick leave due to musculoskeletal disorders. (Occupational Safety and Health Bureau, 2018).
To date, numerous previous studies have investigated musculoskeletal disorders in various worker populations, including office workers, factory workers, handicraft workers, healthcare providers, teachers and agricultural workers (Celik et al., 2018; Chen et al., 2022; Cheung et al., 2021; Phajan et al., 2014; Sopajareeya et al., 2009; Tangkittipaporn & Jiangsathaporn, 2017; Thetkathuek & Meepradit, 2018). However, the prevalence of WRMDs among market vendors in Bangkok, Thailand, remains unclear. Despite this, markets in Thailand play a crucial role in the community as they serve as central hubs for the exchange of products and information. Market vendors, who sell food or goods in these markets, directly engage with buyers by sitting or standing at their shops. According to the National Statistical Office, market vendors constitute the largest group of employees in Bangkok, with 23.13% (1,238,500 individuals) of employed persons working in the wholesale and retail trade industry (National Statistical Office, 2018).
Health risk behaviors encompass actions associated with adverse health consequences, such as non-communicable diseases (Igra & Irwin, 1996) Common health risk behaviors among workers include alcohol consumption, smoking, and insufficient physical activity (John, Hanke & Freyer-Adam, 2018). Alcohol consumption among workers can increase the risk of work accidents and diminish work performance (European Foundation for the Improvement of Living and Working Conditions, 2012). Similarly, insufficient physical activity can lead to various health issues and mortality globally (World Health Organization, 2018)
Furthermore, drug misuse has emerged as a concerning health risk behavior. Drug misuse involves the consumption of medication without a doctor’s prescription or any indication of need. Drug misuse behavior might include taking more than prescribed or labeled, using pharmaceuticals for purposes other than recommended or labeled, or even using drugs belonging to family and friends (Alefan, Halboup & Battah, 2020). If an individual has a headache and takes a pain relief tablet, but their symptoms don’t improve, they might take another dose, thinking, “This will work”. Similarly, someone might take medicine to prevent a fever after being caught in the rain. The impact of improper drug use, including long-term use of medicine, can result in kidney damage. Misusing drugs can contribute to the development of drug resistance. In Thailand, commonly misused medicines include paracetamol, antibiotics, antidepressants, cough and cold relievers, and allergy medicines, as they are readily available at drug stores. Research conducted in the United Kingdom has indicated that overuse of drugs can lead to drug misuse and addiction (Fingleton et al., 2016). The previous study showed NSAIDs, antibiotics, and anti-allergic drugs were the most widely used in Thailand. Minor illnesses and easy access to pharmacies were the most common reasons for self-medication. However, this study found that the participants misunderstood some basic knowledge of the antibiotic drug concepts such as rational drug use or antibiotic stewardship (Chautrakarn, Khumros & Phutrakool, 2021). There are currently no studies describing the prevalence of alcohol consumption, drug misuse, and insufficient physical activity among market vendors in Bangkok. Therefore, the objective of this study was to examine the prevalence of work-related musculoskeletal disorders and health risk behaviors among market vendors.
Materials & Methods
This study employed mixed-methods study design. The quantitative method was used to explore the prevalence of WRMDs and health risk behaviors among market vendors in Bangkok. The qualitative method helped to explain and understand the job characteristics, workstation, market environment and situation that related to WRMDs and health risk behaviors in market-vendors.
The data collection took place in two government-controlled markets located in a business and commercial center area in Bangkok, Thailand. Both markets are categorized as fresh markets, and each comprises over 100 shops. This study collected the data from all of the market vendors in both markets who volunteered and met criteria. The sample size calculation is described in the associated study (Cetthakrikul & Perngparn, 2020). The G-Power program was used with a power of 0.8, based on a satisfactory effect size of 0.64 for the difference in pain scores between groups, which was the primary outcome. After volunteer sampling, the total number of participants was 213. The inclusion and exclusion criteria for participation were as follows: (1) any gender aged 18 years or older; (2) having worked in the market for at least 1 year; (3) not having any diseases that would limit participation in the testing, such as uncontrolled hypertension, heart disease, or neurological problems; and (4) no musculoskeletal disorder involving fibromyalgia, rheumatoid arthritis, lumbar disc prolapse, or other serious traumatic injury. After the researcher provided an explanation of the study’s objectives and protocol to the market vendors to invite their participation. Market vendors who volunteered and met these criteria were recruited for the study.
Among the 148 shops surveyed, 112 shops (75.68%) had one person participate, while 36 shops (24.32%) had more than one person participating. As a result, a total of 213 participants were included in the study.
Data collection utilized two methods. The first method involved qualitative data collection using the direct observation technique. The researcher visited the markets for a total of three days, comprising two weekdays and one weekend, in each market. Observations were made, and information regarding job characteristics, workstations, market environment, and situational aspects was manually recorded between 9:00 am and 5:00 pm.
The second method utilized quantitative data collection through a questionnaire. This questionnaire comprised sections for gathering socio-demographic information, details on health risk behaviors, and a body chart to evaluate areas of pain. The participants were invited to complete a questionnaire. The socio-demographic information included general information such as age, gender, height, weight, and any underlying diseases, as well as working information such as hours and duration of market experience. Health risk behaviors, including alcohol consumption, drug misuse, and lack of regular exercise, were assessed through a questionnaire. Participants provided information on their experience with alcohol, including the duration and frequency of consumption, reasons for drinking, types of alcohol consumed, and daily drinking volume. Regarding drug misuse, participants were asked about their experience with medication, reasons for use, types of medication taken, and the number of pills consumed daily. Exercise habits were evaluated by inquiring about the type, mode, duration, and frequency of exercise, as well as daily sedentary time.
Following the participant’s identification of the pain area on the body chart, this study employed the Nordic Musculoskeletal Questionnaire (NMQ) diagram as a framework to systematically document pain locations within the statistical program for analytical purposes (Kuorinka et al., 1987). The researcher asked the participants to identify areas of the body experiencing musculoskeletal issues. This study categorized the body chart into six areas: neck and upper back, lower back, right arm, left arm, right leg, and left leg. The visual analog scale (VAS) was used for muscle discomfort intensity evaluation (Boonstra et al., 2008). The VAS is a 10-centimeter-long straight line. At one endpoint, a score of zero denoted “no pain”, while a score of ten represented “intolerable pain”. Participants were instructed to mark their perceived pain level on this line. The distance between zero and the marked point determined the participant’s pain intensity (Haefeli & Elfering, 2006). To interpret pain intensity, four levels of pain intensity were identified: no pain (distance = 0 cm), mild pain (distance = 0.1–3.9 cm), moderate pain (distance = 4.0–6.9 cm), and severe pain. Figure 1 showed the tool for rating pain intensity.

Figure 1: Visual Analogue Scale (VAS).
{kind=link}
Additionally, this study evaluated arm and leg muscle flexibility using the Back-scratch test and Chair Sit and Reach test, respectively. Both tests followed guidelines provided by the Sports Authority of Thailand, a unit of the Ministry of Tourism and Sports (Sport Authority of Thailand, 2003). In the Back-scratch test, participants were directed to reach behind their back with one hand positioned over the shoulder and the other hand placed up the middle of the back. The goal was to touch or overlap the fingers of both hands. The distance between the fingers of the two hands was then measured to evaluate arm flexibility. In the Chair Sit and Reach test, participants were seated on the edge of a chair with one leg extended straight in front and the other foot placed flat on the floor. They then leaned forward towards their toes, sliding their hands along the extended leg as far as possible while ensuring the knee remains straight. The distance reached was measured to evaluate leg flexibility. Participants were instructed to practice for the test twice before undergoing three official attempts. The results of the three attempts were averaged and recorded. A negative result was indicated if the fingertips did not touch, while a normal result was recorded if the fingertips either touched or overlapped. The assessors underwent training on utilizing questionnaires and conducting both tests, the Back-scratch test and the Chair Sit and Reach test.
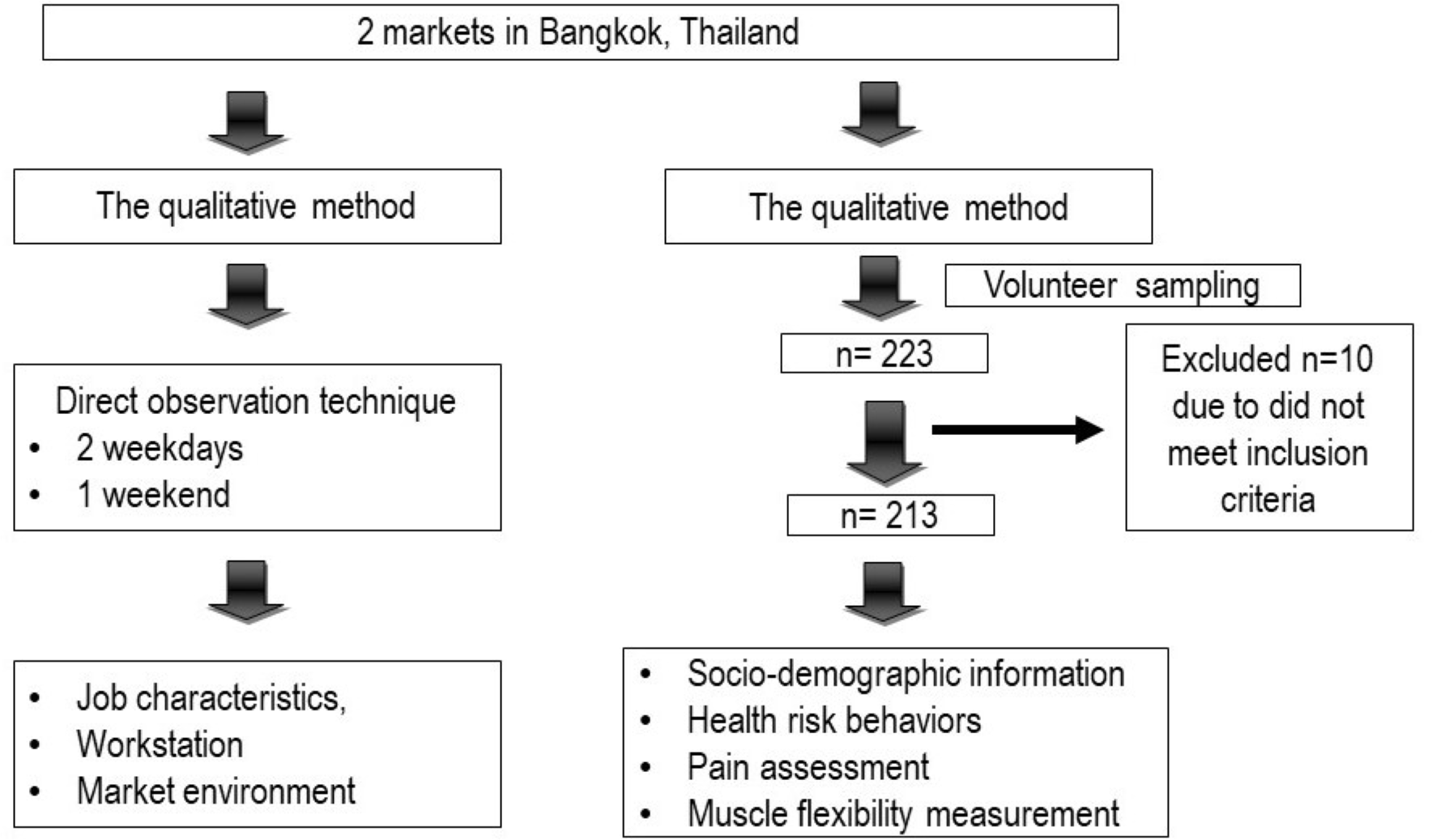
The qualitative data was described and presented through textual descriptions and direct quotations. Quantitative data was analyzed using descriptive statistics, presenting numerical values and percentages. The SPSS program version 22 was employed for data analysis. Prior to data collection, ethical approval was obtained from The Ethics Review Committee for Research Involving Human Research Subjects, Health Science Group, Chulalongkorn University (IRB number 091.1/62). All participants were provided with an information sheet and asked to sign a consent form before participating in the study. Figure 2 shows the flow chart of the study design and the results obtained.
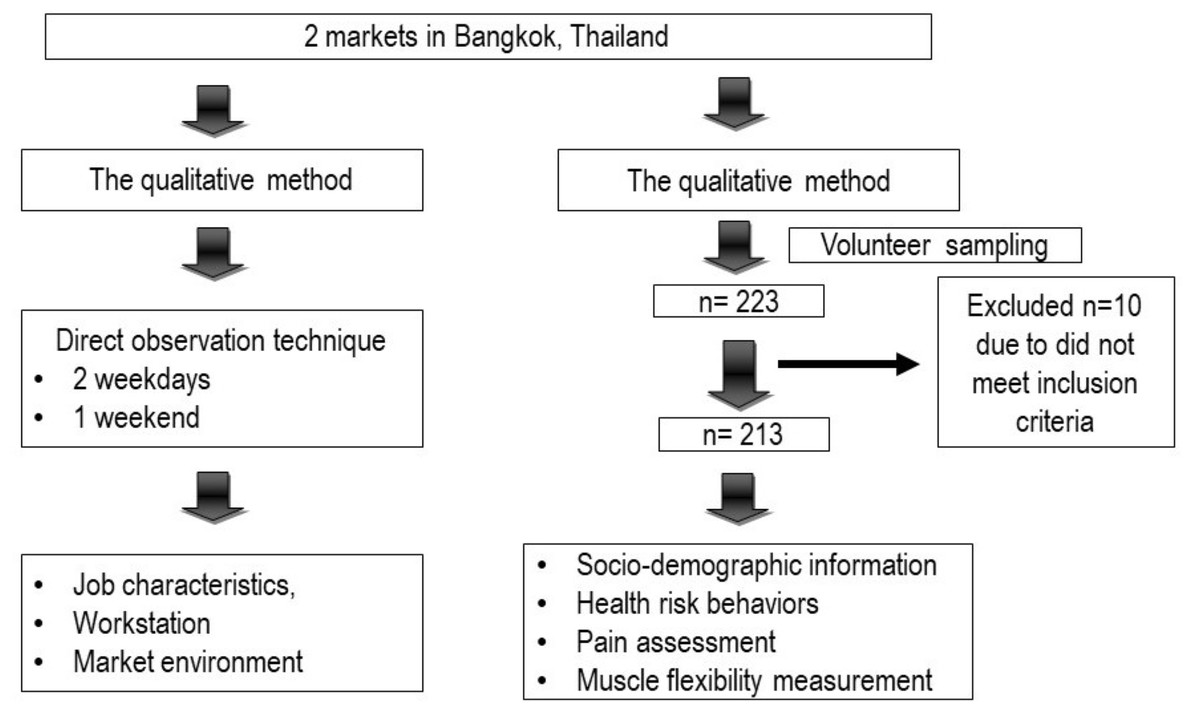
Figure 2: The flow-chart of the data collection.
{kind=link}
Results
Result from qualitative study
Unlike shopping malls, the Thai market is an open area where numerous shops sell a variety of items including cooked food, meat, seafood, fruits, vegetables, and consumer goods. For this study, two markets located in central Bangkok were selected. These markets are easily accessible as they are situated near subway stations. Operating from 6:00 AM to 7:00 PM daily, both markets are managed by a division of the Thai government. They are housed in permanent buildings equipped with amenities such as toilets, sinks, waste collection systems, and parking facilities.
The shop area is 25–30 square meters, consisting of a 100-centimeter height cement counter for placing the products, 4–5 chairs and 1–2 shelves. There are six shop types in the market: (1) meat, (2) seafood, (3) fruit and vegetable, (4) cooked food, (5) dried food, and (6) consumer goods. One market has 126 shops, and another has 608 shops. The highest number is the fruit and vegetable shop and followed by cooked food and consumer goods shop. The shops are divided according to products and are in each zone with the same type of products.
The qualitative study showed the market vendors were female more than male. There were 2–4 market vendors in each shop. Job roles in the market were divided into five main categories: selling goods, arranging shop displays, lifting heavy loads, serving food, and cooking. During the early hours (around 5–6 AM), vendors were busy arranging their shops and preparing food, followed by selling products throughout the day. Peak customer traffic occurred between 8–9 AM and 11 AM–2 PM. Approximately 2 h before closing time, vendors started to pack up their shops. Most vendors were primarily responsible for selling goods and arranging displays, with those in fruit and vegetable shops often involved in heavy lifting. During working hours, vendors tended to prefer sitting or standing still rather than walking, often adopting awkward postures such as working overhead, bending their necks, twisting their trunks, overreaching, or lifting heavy loads.
Result from quantitative study
Population characteristics
A total of participants was 213, male 52 (24.4%) and female 161 (75.6%). More than 90% of participants work in the market every day. Most of the participants were responsible for selling (87.8%) and arranging products (86.4%). 37.6%, 16.9% and 16% of participants were responsible for lifting, serving, and cooking, respectively. Table 1 shows the population characteristic. The average age was 44.73 ± 14.29 years old. 25.4% of them have worked in the market for more than 15 years. About 80% of participants work more than 8 h per day. 87.8% and 77% of participants reported that they always sit or stand continuously for more than 2 h per day.
| Variables | n | % | Mean | SD |
|---|---|---|---|---|
| Gender | ||||
| Male | 52 | 24.4 | ||
| Female | 161 | 75.6 | ||
| Age (year) | 44.73 | 14.29 | ||
| BMI (kg/m2 ) | 24.55 | 4.36 | ||
| <18.5 | 5 | 2.3 | ||
| 18.5–22.9 | 79 | 37.1 | ||
| 23.0–24.9 | 48 | 22.6 | ||
| >25.0 | 81 | 38.0 | ||
| Working duration (years) | 11.34 | 11.22 | ||
| ≤5 | 86 | 40.3 | ||
| 6–10 | 52 | 24.4 | ||
| 11–15 | 21 | 9.9 | ||
| >15 | 54 | 25.4 | ||
| Working hour (h) | 10.46 | 1.92 | ||
| <8 | 14 | 6.57 | ||
| 8–10 | 82 | 38.50 | ||
| 10–12 | 100 | 46.95 | ||
| >12 | 17 | 7.98 | ||
| Prolonged sitting (≥2 h) | 4.83 | 2.71 | ||
| No | 26 | 12.2 | ||
| Yes | 187 | 87.8 | ||
| Prolonged standing (≥2 h) | 4.30 | 2.54 | ||
| No | 49 | 23.0 | ||
| Yes | 164 | 77.0 |
Notes:
- BMI
-
Body mass index
Health risk behaviors
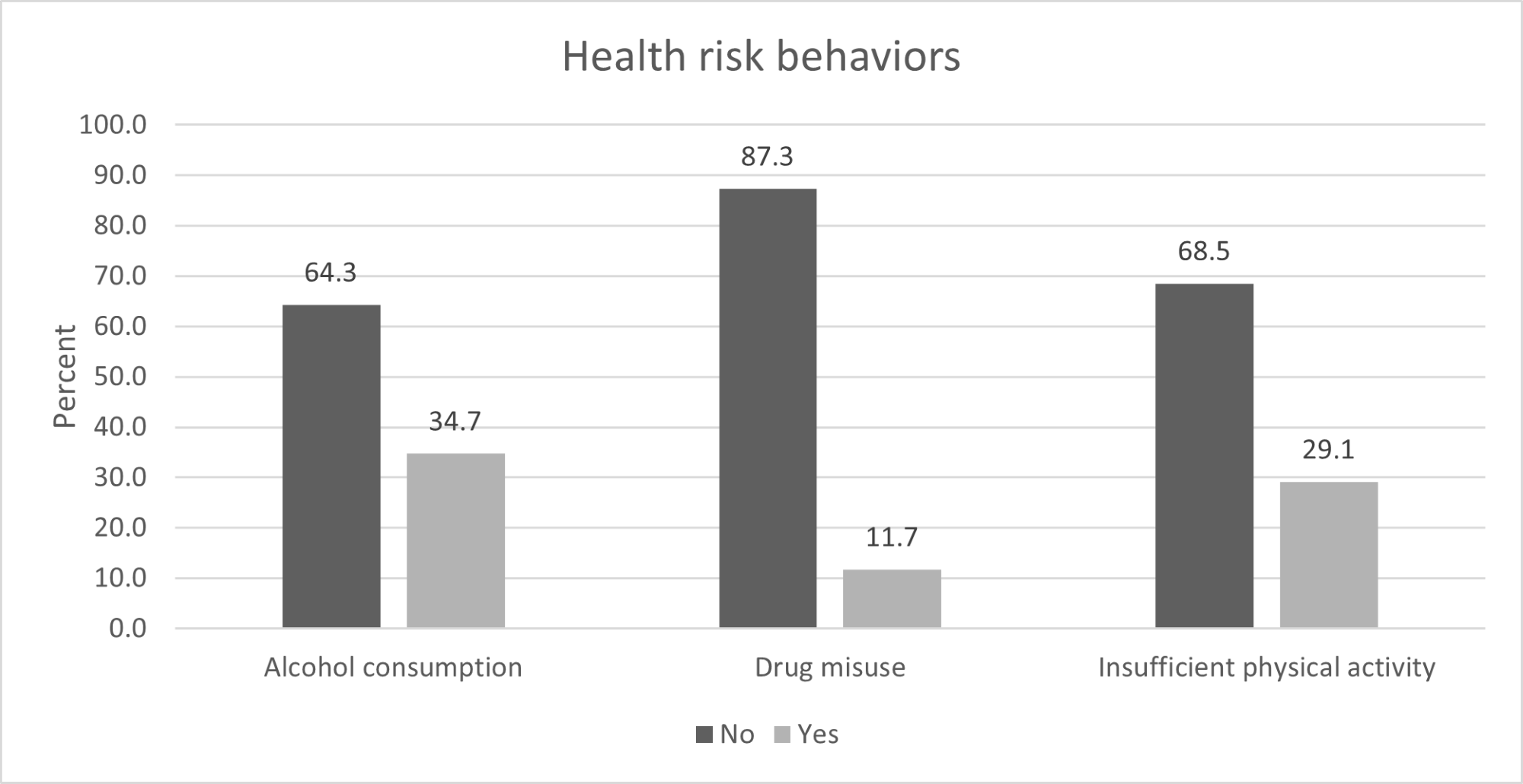
Of the participants, 35.7% (n = 74) reported regular alcohol consumption, with 82.1% (n = 61) of this subset having consumed alcohol within the past month. Among market vendors, relaxation was cited as the primary reason for drinking alcohol, while approximately 10% reported socializing as a motivation. Additionally, 11.7% (n = 25) admitted to drug misuse, with paracetamol being the most commonly used drug, mainly for pain and fever relief. Notably, about 50% of this group (n = 13) took paracetamol without experiencing any symptoms. 68.5% (n = 146), reported insufficient regular exercise, attributing it to reasons such as lack of time, lack of interest, and fatigue from work. Figure 3 provides a visual representation of the percentage of participants engaging in health risk behaviors.
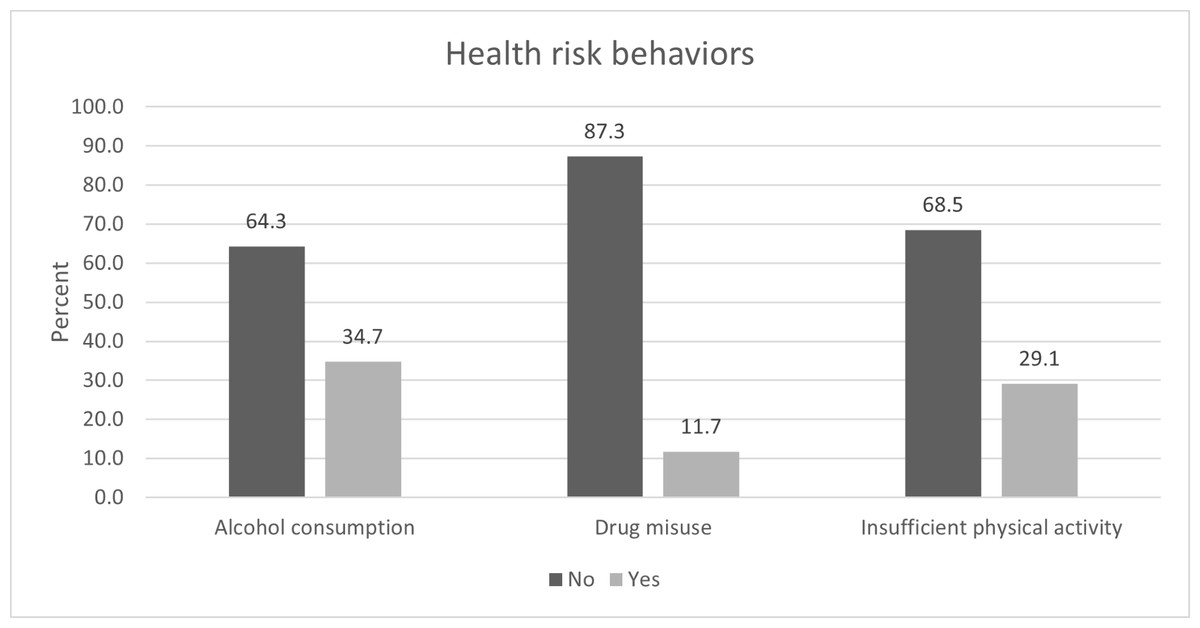
Figure 3: The percentage of participants engaging in health risk behaviors.
{kind=link}
Work-related musculoskeletal disorder in market-vendors
About 70% of all participants (n = 149) had muscle pain within the past 7 days. The right arm region was the majority of pain that occurred among market vendors and followed by left leg, right leg, left arm, lower back and neck and upper back region (34.7%, 31.0%, 30.0%, 28.6%, 21.1% and 10.8% of participant, respectively).
The findings from the Back-scratch test and Chair Sit and Reach test indicated that 64.3% of the sampled market vendors (n = 137) exhibited a lack of muscle flexibility in at least one limb. Nearly half of this demographic displayed negative results in both arms. Furthermore, the analysis revealed that arm muscles tended to have less flexibility compared to leg muscles within the market vendor group. Table 2 provides the average muscle flexibility values for each limb.
| Muscle flexibility (cm) | Normal | Negative result | Mean | SD | ||
|---|---|---|---|---|---|---|
| Region | n | % | n | % | ||
| Right arm muscle | 121 | 56.8 | 92 | 43.2 | −3.13 | 8.03 |
| Left arm muscle | 89 | 41.8 | 124 | 58.2 | −5.99 | 9.59 |
| Right leg muscle | 181 | 85 | 32 | 15.0 | 1.42 | 7.26 |
| Left leg muscle | 179 | 84 | 34 | 16.0 | 1.31 | 7.86 |
Notes:
Normal = the gap between fingertips was 0 cm or greater.
Negative result = The gap between the fingertips was less than 0 cm.
In this study, the body region was divided into six areas: (1) neck and upper back, (2) lower back, (3) right arm, (4) left arm, (5) right leg, and (6) left leg. The findings revealed that the right arm area had the highest prevalence of muscle pain within the past seven days. Additionally, more than 60% of participants who experienced muscle pain within this timeframe reported that the degree of pain was moderate across all areas. Table 3 presented the frequency and degree of muscle pain within past 7 days.
| Self-report muscle pain | n(%) | Pain area | |||||
|---|---|---|---|---|---|---|---|
| Neck and upper back | Lower back | Right arm | Left arm | Right leg | Left leg | ||
| No pain | n | 190 | 168 | 139 | 152 | 149 | 147 |
| % | 89.2 | 78.9 | 65.3 | 71.4 | 70 | 69 | |
| Pain | n | 23 | 45 | 74 | 61 | 64 | 66 |
| % | 10.8 | 21.1 | 34.7 | 28.6 | 30 | 31 | |
| • Mild pain (score = 1–3) | n | 2 | 6 | 9 | 8 | 6 | 8 |
| % | 8.7 | 13.3 | 12.2 | 13.1 | 9.4 | 12.1 | |
| • Moderate pain (score = 4–6) | n | 16 | 32 | 50 | 40 | 43 | 38 |
| % | 69.6 | 71.1 | 67.6 | 65.6 | 67.2 | 57.6 | |
| • Severe pain (score = 7–10) | n | 5 | 7 | 15 | 13 | 15 | 20 |
| % | 21.7 | 15.6 | 20.3 | 21.3 | 23.4 | 30.3 | |
Work-related musculoskeletal disorders and health risk behaviors
The study uncovered that among the 74 participants who consumed alcohol, 51 reported experiencing muscle pain within seven days, and 40 exhibited poor muscle flexibility. Sixteen of the twenty-five participants who had drug misuse experienced muscle pain within seven days, while twenty out of twenty-five demonstrated reduced muscle flexibility. Additionally, among the 146 participants who reported a lack of regular exercise, 98 experienced muscle pain in the past seven days, while 93 exhibited a lack of muscle flexibility. Table 4 showed the summarizes of health risk behaviors, the presence of muscle pain in the past 7 days, and the results of muscle flexibility tests.
| Health risk behaviors | Had muscle pain in past 7 days | Total | Muscle flexibility | Total | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| No | Yes | Normal | Negative result | ||||||||
| n | % | n | % | n | % | n | % | ||||
| Alcohol consumption | No | 41 | 19.43 | 96 | 45.5 | 137 | 42 | 19.91 | 95 | 45.02 | 137 |
| Yes | 23 | 10.9 | 51 | 24.17 | 74 | 34 | 16.11 | 40 | 18.96 | 74 | |
| Total | 64 | 30.33 | 147 | 69.67 | 211 | 76 | 36.02 | 135 | 63.98 | 211 | |
| Drug misused | No | 55 | 26.07 | 131 | 62.09 | 186 | 71 | 33.65 | 115 | 54.5 | 186 |
| Yes | 9 | 4.27 | 16 | 7.58 | 25 | 5 | 2.37 | 20 | 9.48 | 25 | |
| Total | 64 | 30.34 | 147 | 69.67 | 211 | 76 | 36.02 | 135 | 63.98 | 211 | |
| Lack of regular exercise | No | 15 | 7.21 | 47 | 22.60 | 62 | 22 | 10.58 | 40 | 19.23 | 62 |
| Yes | 48 | 23.08 | 98 | 47.12 | 146 | 53 | 25.48 | 93 | 44.71 | 146 | |
| Total | 63 | 30.29 | 145 | 69.71 | 208 | 75 | 36.06 | 133 | 63.94 | 208 | |
Discussion
According to the qualitative study, the result illustrated that market vendors had static muscular work in prolonged sitting and standing. Almost of them were in an awkward posture, for example, working overhead, bending neck, twisting trunk, overreaching, or lifting heavy load. These were risk factors of WRMDs. The prolonged static position can result in muscle discomfort or fatigue because the muscles must work to maintain the position (Canadian Centre for Occupational Health and Safety, 2014). Awkward posture can lead to musculoskeletal disorders such as muscle strain, ligament sprain, muscle pain or fatigue easier than normal position. The injury often occurs because these postures are near the limit of range of motion (ROM). Moreover, the pain intensity caused by a posture will depend on how far from an anatomical posture and its duration (European Agency for Safety and Health at Work, 2008).
The result from qualitative study is related to quantitative study. Arms and legs regions were majority of pain occurred among market vendors in this study. The main reason was the job characteristics. Leg pain in this study was attributed to prolonged standing, while arm pain was linked to repetitive arm movements. Seventy-seven percent of participants reported enduring prolonged standing during their working hours, with an average standing time of 4.3 h per day. According to literature review, prolonged standing exceeding 2 h can induce muscle discomfort, fatigue, and pain in the back, legs, and feet (Azizzati et al., 2013). Similarly, repetitive arm movements resulted in arm pain due to the musculoskeletal structure of the arm being subjected to repetitive strain, leading to muscle fatigue and potential injury (Canadian Centre for Occupational Health and Safety, 2014; European Agency for Safety and Health at Work, 2008). The common area of WRMDs among the market vendors in this study differed from the previous studies. Numerous prior studies have investigated musculoskeletal disorders among workers in Thailand, including factory laborers, handicraft workers, healthcare providers, and agricultural workers. The findings indicated that the pain areas varied across different types of workers, attributable to their distinct job responsibilities. The most prevalent area of WRMDs among factory workers was the lower back (28%), followed by the neck (24%) (Thetkathuek & Meepradit, 2018). In handicraft workers, the most common WRMDs area was the upper back (86.6%), followed by the shoulders (78.8%) (Tangkittipaporn & Jiangsathaporn, 2017). Among healthcare providers, the lower back was the most affected area (45.7%) (Sopajareeya et al., 2009), followed by the neck (28.5%). Additionally, agricultural workers predominantly experienced WRMDs in the lower back (58.7%), followed by the shoulders (42.96%) (Phajan et al., 2014).
The pain experienced by market vendors differs from that of individuals in other occupations due to distinct job characteristics. Market vendors primarily stand at their shops to directly engage with buyers, repeatedly moving their arms for selling and arranging products. This is unlike office workers, who often experience neck, shoulder, and lower back pain due to prolonged sitting and increased computer usage (Celik et al., 2018), or handicraft workers, who may exhibit a high percentage of upper back pain because of static and awkward postures, such as bending down the head and holding arms upward, or sitting on the floor without back support (Tangkittipaporn & Jiangsathaporn, 2017). Additionally, teachers in primary and secondary schools may suffer from lower back and neck pain as a result of prolonged sitting with forward head tilting (Grabara, 2023).
Working in the market entails a heavy workload and long hours. The average working hours were recorded at 10.46 ± 1.92 h per day, surpassing the average for workers in Thailand. Consequently, 35% of the participants reported regular alcohol consumption, attributing it to the belief that alcohol aids in alleviating fatigue from work. Consequently, they often indulge in drinking after completing their work shifts or before bedtime, often in the company of friends or family. The qualitative data revealed insights from market vendors, with some stating, “I drink alcohol every day because it helps me sleep well, and I wake up feeling refreshed in the morning”. Additionally, another vendor mentioned, “I drink alcohol with my friends after finishing work; it helps me relax and forget about the problems from my work”. In the same way, the previous study showed that the indicators of alcohol use in workplace were long working hour, shift work, high risk of injury at work, and high work load (Stockwell et al., 2005). Approximately 10% of participants admitted to taking medication without exhibiting any signs or symptoms of illness. This behavior stemmed from their reluctance to miss work for doctor visits. For instance, a 45-year-old female stated, “I took two tablets of paracetamol yesterday because I don’t want to be sick”. Similarly, a 47-year-old male mentioned, “I often take paracetamol when I get a headache”, while a 56-year-old female reported, “I took a pain relief pill to prevent shoulder pain because I lifted many boxes two days ago”. Additionally, 68% of participants reported a lack of regular exercise, echoing findings from the National Statistical Office. According to their report, the reasons for Thai people not exercising include: 39.7% citing no time for exercise, 31.1% lacking interest, 25.1% feeling tired from work, and 1.4% lacking exercise equipment (National Statistical Office, 2011). Furthermore, many participants expressed feeling pressed for time and cited financial constraints as primary barriers to physical activity.
This study revealed that nearly all participants experiencing a lack of regular exercise also encountered muscle pain and poor muscle flexibility. This correlation may suggest an association between muscle pain and physical activity levels. In a previous study (Grabara, 2023), it was discovered that participants with more WRMDs tended to participate less in vigorous physical activity (VPA) and total physical activity in comparison to those experiencing fewer painful areas of the body. Furthermore, the findings revealed a negative correlation between pain intensity and engagement in physical activity, particularly moderate physical activity (MPA).
The market vendors in this study reported using alcohol and medications like paracetamol or pain relief pills, believing that alcohol could alleviate tiredness and these medicines could either expedite recovery or prevent unpleasant symptoms such as muscle pain or discomfort. Therefore, we deduced that had muscle pain and decreased muscle flexibility could serve as a contributing factor to alcohol consumption and drug misuse among market vendors. This conclusion finds support in previous studies, which have demonstrated a close relationship between musculoskeletal pain and alcohol use. Specifically, these studies have shown that individuals who frequently consume alcohol tend to report higher incidences of neck and shoulder pain compared to those who do not drink alcohol (Chen et al., 2022).
This study represents the first exploration into the prevalence of WRMDs and health risk behaviors among market vendors in Thailand. Market vendors constitute the predominant workforce within Bangkok’s retail sector. Statistics from the National Statistical Office reveal that around 23.13% (1,238,500 individuals) of employed individuals in Bangkok are employed in the wholesale and retail trade industry (National Statistical Office, 2018). However, the limitations of this study include the presence of numerous risk factors associated with WRMDs, such as workplace conditions, the work environment, and psychological factors, which warrant further investigation. Additionally, other health risk factors prevalent in this group, such as smoking and sleeping disorders, were not addressed in this study, and should be explored in future research. Moreover, this study exclusively surveyed work-related musculoskeletal disorders and health risk behaviors among market vendors solely in fresh markets in urban areas of Bangkok. Thus, further research should extend its scope to include other job sectors or areas for a more comprehensive understanding.
Conclusions
This study revealed that market vendors often engaged in static muscular work while enduring prolonged periods of both sitting and standing, frequently assuming awkward postures. The majority of pain among this group was concentrated in the right arm and both legs regions. Market vendors commonly turned to alcohol and medications like paracetamol or pain relief pills, believing that alcohol could alleviate tiredness and these medicines could facilitate a quicker recovery or prevent unpleasant symptoms. Additionally, over 50% of them did not engage in regular exercise. These findings provide valuable insights for developing targeted campaigns aimed at preventing work-related musculoskeletal disorders and addressing health risk behaviors among market vendors. Such campaigns should be tailored to the specific needs of this group.